Вам также может понравиться
- Management of Hemostasis and Coagulopathies for Surgical and Critically Ill Patients: An Evidence-Based ApproachОт EverandManagement of Hemostasis and Coagulopathies for Surgical and Critically Ill Patients: An Evidence-Based ApproachРейтинг: 5 из 5 звезд5/5 (1)
- Blood Bank Review 2019 PDFДокумент613 страницBlood Bank Review 2019 PDFCuddles Pingoy100% (1)
- Blood and Blood ProductsДокумент52 страницыBlood and Blood Productswellawalalasith100% (1)
- Chapter 32 Assessment of Hematologic Function and Treatment ModalitiesДокумент19 страницChapter 32 Assessment of Hematologic Function and Treatment ModalitiesAira Anne Tonee Villamin100% (3)
- Blood AnalysisДокумент4 страницыBlood AnalysisSuman Malik SehrawatОценок пока нет
- Therapeutic Apheresis Guideline FINALVERSION7 THAPRIL15Документ47 страницTherapeutic Apheresis Guideline FINALVERSION7 THAPRIL15RalucaОценок пока нет
- The Coagulation ConsultДокумент284 страницыThe Coagulation ConsultDaniela Franco HОценок пока нет
- Transfusión IntraoperatoriaДокумент24 страницыTransfusión IntraoperatoriaGiovany Salinas100% (1)
- Clinical Use PT and APTTДокумент25 страницClinical Use PT and APTTMustakim DuharingОценок пока нет
- Managing Coagulopathy ICUДокумент38 страницManaging Coagulopathy ICUMirabela Colac100% (1)
- Practice Guidelines For Perioperative Blood Management An Updated Report by The American Society of Anesthesiologists Task Force OnДокумент13 страницPractice Guidelines For Perioperative Blood Management An Updated Report by The American Society of Anesthesiologists Task Force OnMadalina TalpauОценок пока нет
- Massive Transfusion ProtocolДокумент11 страницMassive Transfusion ProtocolAlaa Abdelmoaty OmranОценок пока нет
- 7: Effective Transfusion in Surgery and Critical CareДокумент16 страниц7: Effective Transfusion in Surgery and Critical CareNick-Hugh Sean WisdomОценок пока нет
- Nefrología CríticaДокумент10 страницNefrología CríticaDobson Flores AparicioОценок пока нет
- BR J Haematol - 2022 - Stanworth - A Guideline For The Haematological Management of Major Haemorrhage A British SocietyДокумент14 страницBR J Haematol - 2022 - Stanworth - A Guideline For The Haematological Management of Major Haemorrhage A British SocietyRicardo Victor PereiraОценок пока нет
- A Compendium of Tranfusion Prectice Guidelines ARC Edition 4.0 Jan 2021Документ75 страницA Compendium of Tranfusion Prectice Guidelines ARC Edition 4.0 Jan 2021H Stuard B CocОценок пока нет
- Massive Transfusion Protocol 2017Документ9 страницMassive Transfusion Protocol 2017RosОценок пока нет
- Massive Transfusion - StatPearls - NCBI BookshelfДокумент6 страницMassive Transfusion - StatPearls - NCBI Bookshelfsadam sodomОценок пока нет
- 7 3 Transfusion Management of Major HaemorrhageДокумент6 страниц7 3 Transfusion Management of Major HaemorrhageKoas Neuro UnpattiОценок пока нет
- Santoso2005Документ11 страницSantoso2005ayubahriОценок пока нет
- Review Article Permissive Hypotensive Resuscitation - An Evolving Concept in TraumaДокумент3 страницыReview Article Permissive Hypotensive Resuscitation - An Evolving Concept in TraumareioctabianoОценок пока нет
- Br.J.Anaesth. 2013 Pham I71 82Документ13 страницBr.J.Anaesth. 2013 Pham I71 82tri_budi_20Оценок пока нет
- Optimal Fluid Therapy For Traumatic Hemorrhagic ShockДокумент22 страницыOptimal Fluid Therapy For Traumatic Hemorrhagic ShocksamuelОценок пока нет
- Upper GI BleedДокумент8 страницUpper GI BleedbbyesОценок пока нет
- Massive Transfusion and Massive Transfusion Protocol: Review ArticleДокумент7 страницMassive Transfusion and Massive Transfusion Protocol: Review Articleabinash chihnaraОценок пока нет
- BJH 13580Документ16 страницBJH 13580ManzoorAlamKhattakОценок пока нет
- BJH 12107Документ12 страницBJH 12107Bernard NazaraОценок пока нет
- Joy 1998Документ9 страницJoy 1998Nguyễn Đức LongОценок пока нет
- IndianJAnaesth563234-2277078 061930Документ4 страницыIndianJAnaesth563234-2277078 061930Eka SetiyaniОценок пока нет
- Terapi CairanДокумент5 страницTerapi CairanZikry SitaniaОценок пока нет
- Platelet Transfusion: A Clinical Practice Guideline From The AABB FreeДокумент6 страницPlatelet Transfusion: A Clinical Practice Guideline From The AABB FreeUJI MUTUОценок пока нет
- Postpartum Hemorrhage: Medical and Minimally Invasive ManagementДокумент33 страницыPostpartum Hemorrhage: Medical and Minimally Invasive ManagementMayrita NamayОценок пока нет
- s13019 020 1084 7Документ10 страницs13019 020 1084 7Shalva BasharuliОценок пока нет
- Anaesthesia - 2018 - Mu OzДокумент14 страницAnaesthesia - 2018 - Mu OzCarp TheodorОценок пока нет
- Evolving Science of Trauma Resus 2021-06-17 17-57-30Документ22 страницыEvolving Science of Trauma Resus 2021-06-17 17-57-30Paulina CastilloОценок пока нет
- Postpartum Hemorrhage - Medical and Minimally Invasive Management - Uptodate FreeДокумент59 страницPostpartum Hemorrhage - Medical and Minimally Invasive Management - Uptodate FreecarolinaОценок пока нет
- Cherukuri Et Al. 2018 - Home Haemodialysis Treatment and Outcomes, Retrospective Analysis of KIHDNEyДокумент10 страницCherukuri Et Al. 2018 - Home Haemodialysis Treatment and Outcomes, Retrospective Analysis of KIHDNEyShareDialysisОценок пока нет
- Massive Hemorrhage ProtocolДокумент19 страницMassive Hemorrhage ProtocolYeseniaОценок пока нет
- An International Consensus Statement On The Management of Postoperative Anaemia After Major Surgical ProceduresДокумент14 страницAn International Consensus Statement On The Management of Postoperative Anaemia After Major Surgical ProceduresEdwin PradanaОценок пока нет
- Evidence and Triggers For The Transfusion of Blood and Blood ProductsДокумент9 страницEvidence and Triggers For The Transfusion of Blood and Blood Productscahaya tinggiОценок пока нет
- Bivalirudin Anticoagulant1Документ6 страницBivalirudin Anticoagulant1walid hassanОценок пока нет
- Thromboelastography: Clinical Application, Interpretation, and Transfusion ManagementДокумент7 страницThromboelastography: Clinical Application, Interpretation, and Transfusion ManagementMarcelliaОценок пока нет
- 3.guideline Massive TransfusionДокумент17 страниц3.guideline Massive Transfusionsadam sodomОценок пока нет
- Guidelines For The Administration of PlateletsДокумент13 страницGuidelines For The Administration of PlateletsAlina AndreiОценок пока нет
- Compendium of Transfusion MedicineДокумент50 страницCompendium of Transfusion MedicineLudmilla MartinsОценок пока нет
- Providing Hemostatic and Blood Conservation For Jehovah's Witness PDFДокумент8 страницProviding Hemostatic and Blood Conservation For Jehovah's Witness PDFJasonОценок пока нет
- Blood Transfusion 2Документ7 страницBlood Transfusion 2omarragabselimОценок пока нет
- MTP2Документ6 страницMTP2Xavier Alexandro Ríos SalinasОценок пока нет
- 2008 Tale of The Seven MaresДокумент9 страниц2008 Tale of The Seven MaresEduardo Alfredo Gutierrez PardoОценок пока нет
- Goal-Directed Fluid Restriction During Brain Surgery: A Prospective Randomized Controlled TrialДокумент7 страницGoal-Directed Fluid Restriction During Brain Surgery: A Prospective Randomized Controlled TrialkenjiОценок пока нет
- Frank 2019Документ15 страницFrank 2019Oliver ArteagaОценок пока нет
- Ultra-Early Tranexamic Acid After Subarachnoid Hemorrhage (ULTRA) : Study Protocol For A Randomized Controlled TrialДокумент7 страницUltra-Early Tranexamic Acid After Subarachnoid Hemorrhage (ULTRA) : Study Protocol For A Randomized Controlled Trialrikadwi20Оценок пока нет
- Antiplatelet Drugs: Mechanisms and Risks of Bleeding Following Cardiac OperationsДокумент18 страницAntiplatelet Drugs: Mechanisms and Risks of Bleeding Following Cardiac OperationsViona PrasetyoОценок пока нет
- Richards JE, Damage Control Resuscitation in Traumatic Hemorrhage, It Is More Than, Anesthesiol 2023Документ13 страницRichards JE, Damage Control Resuscitation in Traumatic Hemorrhage, It Is More Than, Anesthesiol 2023jorge fabregatОценок пока нет
- 2 Aet376Документ12 страниц2 Aet376sadam sodomОценок пока нет
- Metanalisis Elevacion Pasiva de MMIIДокумент11 страницMetanalisis Elevacion Pasiva de MMIImayraОценок пока нет
- Blood Transfusion in Critical Care: Giora Netzer, Richard P Dutton and John R HessДокумент3 страницыBlood Transfusion in Critical Care: Giora Netzer, Richard P Dutton and John R Hessnevermore11Оценок пока нет
- Blood TransfusionДокумент11 страницBlood Transfusionsaid tariqОценок пока нет
- Vox SanguinisДокумент179 страницVox SanguinistristanmunarОценок пока нет
- Perioperative Patient Blood Management To Improve.19Документ10 страницPerioperative Patient Blood Management To Improve.19Reinaldi octaОценок пока нет
- A High Mean Arterial PressureДокумент8 страницA High Mean Arterial Pressureadek07Оценок пока нет
- 14 - Mazandarani2012Документ7 страниц14 - Mazandarani2012TandeanTommyNovenantoОценок пока нет
- GI Bleeding (Text)Документ11 страницGI Bleeding (Text)Hart ElettОценок пока нет
- Continuous Noninvasive Hemoglobin 2019Документ8 страницContinuous Noninvasive Hemoglobin 2019azizk83Оценок пока нет
- Anesthesiology 2015Документ11 страницAnesthesiology 2015The Vancouver SunОценок пока нет
- Decompressive CraniectomyДокумент20 страницDecompressive CraniectomyAnonymous BQM9271ZXОценок пока нет
- Anestesi Pada Operaso Telinga TengahДокумент9 страницAnestesi Pada Operaso Telinga TengahAnonymous BQM9271ZXОценок пока нет
- Gogarten-2010-ESA Guideline Regional and Thrombolytic Agent 2010Документ17 страницGogarten-2010-ESA Guideline Regional and Thrombolytic Agent 2010Anonymous BQM9271ZXОценок пока нет
- Anaesthesia in CKD MAJUДокумент21 страницаAnaesthesia in CKD MAJUAnonymous BQM9271ZXОценок пока нет
- TechTalk Acceptable Minimum Draw VolumeEДокумент2 страницыTechTalk Acceptable Minimum Draw VolumeEARIF AHAMMED PОценок пока нет
- Using TMS Method/factor Gathered and Processed by NDA-PMSED NDA-PMSD9/17/2021 Basic Source: Phil. Statistics AuthorityДокумент1 страницаUsing TMS Method/factor Gathered and Processed by NDA-PMSED NDA-PMSD9/17/2021 Basic Source: Phil. Statistics AuthorityNoreen Guiyab TannaganОценок пока нет
- Bleeding Time QuizДокумент4 страницыBleeding Time QuizJHON JORIES VISMONTEОценок пока нет
- Cryoprecipitate The Current State of KnowledgeДокумент12 страницCryoprecipitate The Current State of KnowledgeAngel Bernardo GutiérrezОценок пока нет
- APTT-SP (Liquid) - 0020006300: Et Al For Identification and Resolution of Out-Of-Control SituationsДокумент3 страницыAPTT-SP (Liquid) - 0020006300: Et Al For Identification and Resolution of Out-Of-Control SituationsCaro ErazoОценок пока нет
- RITM Laboratory Diagnostic Services BrochureДокумент65 страницRITM Laboratory Diagnostic Services BrochureRITM DOH67% (3)
- 2020.03.10 AddendumДокумент2 страницы2020.03.10 AddendumStib BrionesОценок пока нет
- Buffalo BulletinДокумент6 страницBuffalo Bulletinprajakta kuralkarОценок пока нет
- Anaemia in Pregnancy: Klinik Kesihatan Ibu Dan Anak Parit BuntarДокумент10 страницAnaemia in Pregnancy: Klinik Kesihatan Ibu Dan Anak Parit Buntarannurshah05Оценок пока нет
- Unit 1 Serology: A BO and RH D Blood Group PolymorphismsДокумент16 страницUnit 1 Serology: A BO and RH D Blood Group PolymorphismspawanahirwarОценок пока нет
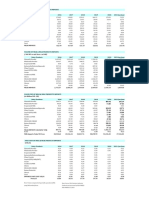
- Laporan Pasien Covid19 Ranap Dan Rajal RSI Darus Syifa SbyДокумент61 страницаLaporan Pasien Covid19 Ranap Dan Rajal RSI Darus Syifa SbyNur HasanahОценок пока нет
- Complete Blood Count (CBC) Test: WBC DifferentialДокумент4 страницыComplete Blood Count (CBC) Test: WBC Differentialchang02Оценок пока нет
- Chap 4 Blood HemoДокумент23 страницыChap 4 Blood HemoDianne GalangОценок пока нет
- Jurnal 1. Koagulasi Dan Golongan DarahДокумент8 страницJurnal 1. Koagulasi Dan Golongan DarahnisrinaОценок пока нет
- Von Willebrand DiseaseДокумент4 страницыVon Willebrand DiseaseJohannah DaroОценок пока нет
- Albumin-Indirect Antiglobulin TestДокумент2 страницыAlbumin-Indirect Antiglobulin TestCatia CorreaОценок пока нет
- Reference: Harmening, D.M. (2012) - Modern Blood Banking & Transfusion Practices. 6 Ed. Pg. 123. F.A. Davis CompanyДокумент2 страницыReference: Harmening, D.M. (2012) - Modern Blood Banking & Transfusion Practices. 6 Ed. Pg. 123. F.A. Davis CompanyMARC AIVIN BEATOОценок пока нет
- Dengue NCPДокумент3 страницыDengue NCPingridОценок пока нет
- Distribution of ABO and RH-D Blood Group Antigens Among Blood Donors in The Amhara Regional State, EthiopiaДокумент11 страницDistribution of ABO and RH-D Blood Group Antigens Among Blood Donors in The Amhara Regional State, EthiopiaSely wulan widya ningsihОценок пока нет
- The Red Cell Histogram and The Dimorphic Red Cell PopulationДокумент9 страницThe Red Cell Histogram and The Dimorphic Red Cell PopulationAlan Dwi SaputraОценок пока нет
- Blood Banking Procedures Notes Final PDFДокумент7 страницBlood Banking Procedures Notes Final PDFAhmed AliОценок пока нет
- Blood Bank Notes: History: de Motu Cordis Paved The Way For An Entirely New Arena ofДокумент3 страницыBlood Bank Notes: History: de Motu Cordis Paved The Way For An Entirely New Arena ofRojane Camille A. ValdozОценок пока нет
- Management of Patients With Nonmalignant Hematologic DisordersДокумент97 страницManagement of Patients With Nonmalignant Hematologic DisordersJulia Rae Delos SantosОценок пока нет
- Blood TypingДокумент3 страницыBlood TypingNoriz Ember DominguezОценок пока нет
- Study of The Ratio of Cross-Matching To Transfusio PDFДокумент7 страницStudy of The Ratio of Cross-Matching To Transfusio PDFampratikna 14Оценок пока нет