Вам также может понравиться
- Using Casemix System for Hospital Reimbursement in Social Health Insurance Programme: Comparing Casemix System and Fee-For-Service as Provider Payment MethodОт EverandUsing Casemix System for Hospital Reimbursement in Social Health Insurance Programme: Comparing Casemix System and Fee-For-Service as Provider Payment MethodОценок пока нет
- Health Insurance SchemeДокумент10 страницHealth Insurance SchemeKailash NagarОценок пока нет
- Nonfinancial Defined Contribution Pension Schemes in a Changing Pension World: Volume 1, Progress, Lessons, and ImplementationОт EverandNonfinancial Defined Contribution Pension Schemes in a Changing Pension World: Volume 1, Progress, Lessons, and ImplementationОценок пока нет
- Thailand'S Universal Health Coverage: Dr. Thaworn Sakunphanit MD., FRCPT, Ba (Econ), Msc. (Social Policy Financing)Документ17 страницThailand'S Universal Health Coverage: Dr. Thaworn Sakunphanit MD., FRCPT, Ba (Econ), Msc. (Social Policy Financing)IManОценок пока нет
- Social Health Protection Toward UHC in Lao PDRДокумент16 страницSocial Health Protection Toward UHC in Lao PDRADBI EventsОценок пока нет
- Caring for Others Amid Covid-19: Recruitment and Retention in Long Term CareОт EverandCaring for Others Amid Covid-19: Recruitment and Retention in Long Term CareОценок пока нет
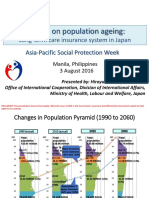
- APSP - Session 9A - Hiroyuki Yamaya - MHLWДокумент8 страницAPSP - Session 9A - Hiroyuki Yamaya - MHLWKristine PresbiteroОценок пока нет
- Pharmacy Practice IДокумент157 страницPharmacy Practice ISalahadinОценок пока нет
- 1 DR.N.S.R Chandraprasad, Chairman & MD, National Insurance Company - Healthcare Insurance Past, Present & FutureДокумент46 страниц1 DR.N.S.R Chandraprasad, Chairman & MD, National Insurance Company - Healthcare Insurance Past, Present & FutureAkshayОценок пока нет
- Unit 5 Social Security SchemesДокумент58 страницUnit 5 Social Security SchemesKanwaljeet SinghОценок пока нет
- Primary Health Care The BuildingДокумент4 страницыPrimary Health Care The BuildingZurОценок пока нет
- Health Systems in Transition People's Republic of China Health System ReviewДокумент30 страницHealth Systems in Transition People's Republic of China Health System Review卜梦然Оценок пока нет
- Occupationalhealth 180403094034Документ58 страницOccupationalhealth 180403094034shravaniОценок пока нет
- Health SchemesДокумент70 страницHealth SchemesA J FathimaОценок пока нет
- Ayushman BharatДокумент18 страницAyushman BharatNeethu VincentОценок пока нет
- Universal Health Coverage: Case of MalaysiaДокумент38 страницUniversal Health Coverage: Case of MalaysiaADBI Events100% (5)
- Healthcare System in Vietnam - NganДокумент18 страницHealthcare System in Vietnam - NganhksonnganОценок пока нет
- Moving Towards Universal Health Access in Indonesia: Dr. Nafsiah Mboi, Sp.A, MPH Minister of Health Republic of IndonesiaДокумент32 страницыMoving Towards Universal Health Access in Indonesia: Dr. Nafsiah Mboi, Sp.A, MPH Minister of Health Republic of Indonesiarani fajraОценок пока нет
- Kakoloti - Key Issues Facing The Health Sector in The Next Five Years (2007)Документ19 страницKakoloti - Key Issues Facing The Health Sector in The Next Five Years (2007)Dinesh PatelОценок пока нет
- Ex-Servicemen Contributory Health Scheme: ContributionsДокумент2 страницыEx-Servicemen Contributory Health Scheme: ContributionsKashishОценок пока нет
- Paper41 Many ActsДокумент17 страницPaper41 Many ActsSwati GargОценок пока нет
- Case of Japan: Effectiveness of Universal Health InsuranceДокумент22 страницыCase of Japan: Effectiveness of Universal Health InsuranceADBI Events100% (1)
- Esi Scheme in Tamil Nadu: Directorate of Medical and Rural Health Services (Esi) Chennai - 6Документ33 страницыEsi Scheme in Tamil Nadu: Directorate of Medical and Rural Health Services (Esi) Chennai - 6Ash MohОценок пока нет
- Ayushman Bharat YojanaДокумент28 страницAyushman Bharat YojanaParth VasaveОценок пока нет
- UK Experience in Managing NHS From A Public Policymanagement Perspective (GD2 10-05-17)Документ40 страницUK Experience in Managing NHS From A Public Policymanagement Perspective (GD2 10-05-17)Yofintya R.S.P.25Оценок пока нет
- HCDSДокумент35 страницHCDSKrishnaveni MurugeshОценок пока нет
- Review of National Health Mission & SDGS: Presented By: Gargi Pandey JR-2Документ114 страницReview of National Health Mission & SDGS: Presented By: Gargi Pandey JR-2Gargi pandeyОценок пока нет
- Pembiayaan Kesehatan UHCДокумент43 страницыPembiayaan Kesehatan UHCGenre PesselОценок пока нет
- Ealth Nsurance: Chapter ReviewДокумент222 страницыEalth Nsurance: Chapter ReviewYi QingОценок пока нет
- Moving Towards Universal Health Access in Indonesia: Dr. Nafsiah Mboi, Sp.A, MPH Minister of Health Republic of IndonesiaДокумент32 страницыMoving Towards Universal Health Access in Indonesia: Dr. Nafsiah Mboi, Sp.A, MPH Minister of Health Republic of IndonesiamochkurniawanОценок пока нет
- To Increase The Accessibility To Essential Medicines in ThailandДокумент38 страницTo Increase The Accessibility To Essential Medicines in ThailandADBI EventsОценок пока нет
- Master Plan RSHДокумент15 страницMaster Plan RSHBispro VivamedikaОценок пока нет
- My Term Paper FinalДокумент10 страницMy Term Paper FinalGokool KiniОценок пока нет
- Social Health Insurance in India Current ScenarioДокумент22 страницыSocial Health Insurance in India Current ScenarioRohit MalviyaОценок пока нет
- Australia - International Health Care System ProfilesДокумент10 страницAustralia - International Health Care System ProfilesAboubacar SompareОценок пока нет
- Reform of The Chinese Health Care Financing System: Gu Xing-Yuan" A, Tang Sheng-LanbДокумент11 страницReform of The Chinese Health Care Financing System: Gu Xing-Yuan" A, Tang Sheng-LanbAswarОценок пока нет
- Vermont Report Recommends Single Payer System - Presentation To The State LegislatureДокумент33 страницыVermont Report Recommends Single Payer System - Presentation To The State LegislatureRich ElmoreОценок пока нет
- OCOpen Source HMISenabled UHCmonitoringandevaluationin BurundianhospitalsДокумент16 страницOCOpen Source HMISenabled UHCmonitoringandevaluationin BurundianhospitalsPhally UmОценок пока нет
- 4 Ochoa Naples1Документ53 страницы4 Ochoa Naples1martinsmicaelribeiroОценок пока нет
- Switzerland's Health Care System: Jaroslav Molik, Swiss Reinsurance CompanyДокумент29 страницSwitzerland's Health Care System: Jaroslav Molik, Swiss Reinsurance CompanyShafira TamaraОценок пока нет
- Health Insurance: Awareness, Utilization, and Its Determinants Among The Urban Poor in Delhi, IndiaДокумент8 страницHealth Insurance: Awareness, Utilization, and Its Determinants Among The Urban Poor in Delhi, IndiaY S KusumaОценок пока нет
- Schemes (Part 4) - HealthДокумент17 страницSchemes (Part 4) - HealthbwerОценок пока нет
- Health Insurance: DR - Bharat PaulДокумент74 страницыHealth Insurance: DR - Bharat PaulAnonymous So5qPSnОценок пока нет
- Healthcare PoliciesДокумент7 страницHealthcare PoliciesDanish RaisОценок пока нет
- The Feasibility of A Community Based Health Insurance (CBHI) at Wayanad, KeralaДокумент43 страницыThe Feasibility of A Community Based Health Insurance (CBHI) at Wayanad, Keralatapz07Оценок пока нет
- NHI4UHC Day 1 Session 1 UHC in ThailandДокумент26 страницNHI4UHC Day 1 Session 1 UHC in ThailandADB Health Sector GroupОценок пока нет
- Thirty Years of National Health Insurance in South Korea: Lessons For Achieving Universal Health Care CoverageДокумент10 страницThirty Years of National Health Insurance in South Korea: Lessons For Achieving Universal Health Care CoverageMirsa Octavia WardayaniОценок пока нет
- Asuransi Kesehatan Di ChinaДокумент12 страницAsuransi Kesehatan Di ChinaHafselОценок пока нет
- Student ExchangeДокумент39 страницStudent Exchangerani arsantiОценок пока нет
- Intl Profiles FranceДокумент5 страницIntl Profiles FranceJesse M. MassieОценок пока нет
- Yankesja Sesi 3 Kelompok 11Документ27 страницYankesja Sesi 3 Kelompok 11FORDОценок пока нет
- Leadership & ManagementДокумент44 страницыLeadership & ManagementShaheed HayangОценок пока нет
- Intro To Healthcare and Ehealth in The Philippines: Kristine Mae P. Magtubo MD MPMДокумент17 страницIntro To Healthcare and Ehealth in The Philippines: Kristine Mae P. Magtubo MD MPMGlenice JoyОценок пока нет
- 20171229-Tss-Genel-Bakis-En TOBB PDFДокумент69 страниц20171229-Tss-Genel-Bakis-En TOBB PDFsbulenterisОценок пока нет
- Employees' State Insurance SchemeДокумент90 страницEmployees' State Insurance SchemelordavengerОценок пока нет
- March 16-31, English, My Notes by DR KhanДокумент32 страницыMarch 16-31, English, My Notes by DR KhanKsg IndiaОценок пока нет
- Universal Health Coverage (UHC) : Challenges & Solutions, What Can We Learn From Indonesia?Документ33 страницыUniversal Health Coverage (UHC) : Challenges & Solutions, What Can We Learn From Indonesia?ADBI EventsОценок пока нет
- Accenture Base Policy Coverages..Документ3 страницыAccenture Base Policy Coverages..Mahesh M.Оценок пока нет
- Evaluation of Pilot SSK ProgramДокумент77 страницEvaluation of Pilot SSK ProgramchatgptfnfОценок пока нет
- KFC To Release Gaming Console That Heats ChickenДокумент4 страницыKFC To Release Gaming Console That Heats ChickenElly Nu'ma ZahrotiОценок пока нет
- Underwater Sculpture Park To Open in MiamiДокумент4 страницыUnderwater Sculpture Park To Open in MiamiElly Nu'ma ZahrotiОценок пока нет
- Ielts Task 1Документ14 страницIelts Task 1Elly Nu'ma ZahrotiОценок пока нет
- Thailand: General InformationДокумент1 страницаThailand: General InformationElly Nu'ma ZahrotiОценок пока нет
- AJ Hoge Rule 1 PDFДокумент7 страницAJ Hoge Rule 1 PDFElly Nu'ma Zahroti100% (1)
- You Have The DREAM. We Have The ResourcesДокумент6 страницYou Have The DREAM. We Have The ResourcesElly Nu'ma ZahrotiОценок пока нет
- Factsheet Life Sciences & Health in ThailandДокумент4 страницыFactsheet Life Sciences & Health in ThailandElly Nu'ma ZahrotiОценок пока нет
- Perbandingan Silabus Univ SwedenДокумент1 страницаPerbandingan Silabus Univ SwedenElly Nu'ma ZahrotiОценок пока нет
- Teori OrganisasiДокумент14 страницTeori OrganisasiElly Nu'ma ZahrotiОценок пока нет
- PHC 3440 Global Public Health Syllabus SpringДокумент7 страницPHC 3440 Global Public Health Syllabus SpringElly Nu'ma ZahrotiОценок пока нет
- Master's in Public Health: Programme OverviewДокумент2 страницыMaster's in Public Health: Programme OverviewElly Nu'ma ZahrotiОценок пока нет
- Ngo Org PrinciplesДокумент18 страницNgo Org PrinciplesElly Nu'ma ZahrotiОценок пока нет
- Deutschland Stipendium Hinweise en Important Information For Scholarship ApplicantsДокумент5 страницDeutschland Stipendium Hinweise en Important Information For Scholarship ApplicantsElly Nu'ma ZahrotiОценок пока нет
- Indonesia Health System Review 2017 PDFДокумент329 страницIndonesia Health System Review 2017 PDFElly Nu'ma Zahroti100% (2)
- User Requirement AssessmentДокумент28 страницUser Requirement AssessmentElly Nu'ma ZahrotiОценок пока нет
- Tugas EnglishДокумент5 страницTugas EnglishDien NaОценок пока нет
- World Health OrganizationДокумент35 страницWorld Health OrganizationPrashun PriyadarshiОценок пока нет
- Truenat MTB Leaflet 2Документ2 страницыTruenat MTB Leaflet 2yousra zeidanОценок пока нет
- Worksheet - Causal Arguments (Edited S1 2023)Документ8 страницWorksheet - Causal Arguments (Edited S1 2023)danielОценок пока нет
- Published Immunogenicity and Safety of A Novel Ten-Valent PNДокумент13 страницPublished Immunogenicity and Safety of A Novel Ten-Valent PNIvan GeromeОценок пока нет
- Protecting Yourself When Handling Contaminated Sharps OSHAДокумент2 страницыProtecting Yourself When Handling Contaminated Sharps OSHARaúlОценок пока нет
- 48 - 1 - AYUSH Doctor Job ChartДокумент4 страницы48 - 1 - AYUSH Doctor Job ChartNobel LaureateОценок пока нет
- Abstract Comparison Between Albendazole and MebendazoleДокумент25 страницAbstract Comparison Between Albendazole and MebendazoleluzОценок пока нет
- Quaratine Isolation Center DesignДокумент6 страницQuaratine Isolation Center DesignYeabtsega ZelalemОценок пока нет
- Jsa Radiographic Test RTДокумент1 страницаJsa Radiographic Test RTHussein Adnan Fneish100% (1)
- Cardiometabolic Syndrome: & DR Dhafir A. MahmoodДокумент62 страницыCardiometabolic Syndrome: & DR Dhafir A. MahmoodJacob AlphaОценок пока нет
- Kode Icd X Permenkes No 5 Tahun 2014Документ6 страницKode Icd X Permenkes No 5 Tahun 2014may rosa bintangОценок пока нет
- 1583-Article Text-18610-3-10-20200103Документ10 страниц1583-Article Text-18610-3-10-20200103HendraОценок пока нет
- HealthReformInChina PDFДокумент204 страницыHealthReformInChina PDFJason LiОценок пока нет
- Chief Report 16.08.2019Документ78 страницChief Report 16.08.2019Inez WijayaОценок пока нет
- Choosing Antibiotic Therapy For Severe Community-Acquired PneumoniaДокумент7 страницChoosing Antibiotic Therapy For Severe Community-Acquired PneumoniaJuan Sebastian SuarezОценок пока нет
- Health Systems in IndiaДокумент39 страницHealth Systems in IndiaKamali MuthuОценок пока нет
- Matriz CargaДокумент80 страницMatriz CargaRodnei MacedoОценок пока нет
- Epidemiology and Prevention of Diabetes MellitusДокумент38 страницEpidemiology and Prevention of Diabetes MellitusMir Asfandyar HothОценок пока нет
- Name of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesДокумент2 страницыName of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesIvan Matthew SuperioОценок пока нет
- FOOD CONTAMINATION WORKSHEET 2 (Repaired)Документ3 страницыFOOD CONTAMINATION WORKSHEET 2 (Repaired)compilationsОценок пока нет
- CPS BC STI Treatment Guidelines 20112014Документ11 страницCPS BC STI Treatment Guidelines 20112014Maria Teresa SanromanОценок пока нет
- LESSON 2 - Food and NutritionДокумент3 страницыLESSON 2 - Food and NutritionSan Jose, Kyla Mae M.Оценок пока нет
- CERC Introduction PDFДокумент11 страницCERC Introduction PDFIan Lusay Ofendoreyes100% (1)
- CE3040 - L01 - Course Content - 28012023Документ4 страницыCE3040 - L01 - Course Content - 28012023Shanmukesh YadavОценок пока нет
- Intensive Care Unit Issues in Eclampsia and HELLP SyndromeДокумент2 страницыIntensive Care Unit Issues in Eclampsia and HELLP SyndromeYoga Maulana HernowoОценок пока нет
- Self Instructional Training Methods To R 08c89fef PDFДокумент6 страницSelf Instructional Training Methods To R 08c89fef PDFIbu SaniyahОценок пока нет
- TB Control in Garment Factories - DhakaДокумент76 страницTB Control in Garment Factories - DhakaAmandeep SinghОценок пока нет
- Presentation 1Документ9 страницPresentation 1NgsfbsbsfiОценок пока нет
- Gyne Removals SamplexДокумент43 страницыGyne Removals SamplexHa Jae kyeongОценок пока нет
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisОт EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (9)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceОт EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceРейтинг: 4.5 из 5 звезд4.5/5 (15)
- The Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthОт EverandThe Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthОценок пока нет
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineОт EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineОценок пока нет
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicОт EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicОценок пока нет
- The Inescapable Immune Escape PandemicОт EverandThe Inescapable Immune Escape PandemicРейтинг: 5 из 5 звезд5/5 (1)
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsОт EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsРейтинг: 4.5 из 5 звезд4.5/5 (6)
- Sickening: How Big Pharma Broke American Health Care and How We Can Repair ItОт EverandSickening: How Big Pharma Broke American Health Care and How We Can Repair ItРейтинг: 4 из 5 звезд4/5 (9)
- Clean: Overcoming Addiction and Ending America’s Greatest TragedyОт EverandClean: Overcoming Addiction and Ending America’s Greatest TragedyРейтинг: 4 из 5 звезд4/5 (18)
- Heat Wave: A Social Autopsy of Disaster in ChicagoОт EverandHeat Wave: A Social Autopsy of Disaster in ChicagoРейтинг: 4 из 5 звезд4/5 (40)
- The Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryОт EverandThe Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryРейтинг: 4 из 5 звезд4/5 (6)
- Fatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthОт EverandFatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthРейтинг: 4 из 5 звезд4/5 (7)
- Summary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedОценок пока нет
- Environmental Health and Occupational Health & SafetyОт EverandEnvironmental Health and Occupational Health & SafetyРейтинг: 3.5 из 5 звезд3.5/5 (9)
- Profiles of the Vaccine-Injured: "A Lifetime Price to Pay"От EverandProfiles of the Vaccine-Injured: "A Lifetime Price to Pay"Рейтинг: 3.5 из 5 звезд3.5/5 (3)
- Breaking out of the Health Care Abyss: Transformational Tips for Agents of ChangeОт EverandBreaking out of the Health Care Abyss: Transformational Tips for Agents of ChangeОценок пока нет
- The Wuhan Cover-Up: And the Terrifying Bioweapons Arms RaceОт EverandThe Wuhan Cover-Up: And the Terrifying Bioweapons Arms RaceОценок пока нет
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceОт EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceРейтинг: 4.5 из 5 звезд4.5/5 (11)
- Healthy Buildings: How Indoor Spaces Drive Performance and ProductivityОт EverandHealthy Buildings: How Indoor Spaces Drive Performance and ProductivityРейтинг: 5 из 5 звезд5/5 (2)
- The Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanОт EverandThe Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanРейтинг: 4.5 из 5 звезд4.5/5 (12)
- Epic Measures: One Doctor. Seven Billion Patients.От EverandEpic Measures: One Doctor. Seven Billion Patients.Рейтинг: 4 из 5 звезд4/5 (13)
- Mama Might Be Better Off Dead: The Failure of Health Care in Urban AmericaОт EverandMama Might Be Better Off Dead: The Failure of Health Care in Urban AmericaОценок пока нет
- Vaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadОт EverandVaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadРейтинг: 4.5 из 5 звезд4.5/5 (3)