Вам также может понравиться
- Diabetes Type 2 BasicsДокумент44 страницыDiabetes Type 2 BasicsMasunji EmanuelОценок пока нет
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesОт EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesРейтинг: 4 из 5 звезд4/5 (2)
- Diabetes Mellitus in PregnancyДокумент55 страницDiabetes Mellitus in Pregnancyapi-3856051100% (2)
- Ati Endocrine 2016 1Документ6 страницAti Endocrine 2016 1Jamil AhmedОценок пока нет
- NCM 118a Lec 10 Hyperosmolar Hyperglycemic SДокумент4 страницыNCM 118a Lec 10 Hyperosmolar Hyperglycemic SJan Crizza Dale R. FrancoОценок пока нет
- GDMДокумент66 страницGDMpooja singhОценок пока нет
- Diabetes OPD ดีมากกกДокумент5 страницDiabetes OPD ดีมากกกPonpimol Odee BongkeawОценок пока нет
- DM CBLДокумент18 страницDM CBLbpt2Оценок пока нет
- DM in PregДокумент32 страницыDM in Pregbryanpei23Оценок пока нет
- eEMCASE - MAR Letak Rendah Tanpa FistelДокумент22 страницыeEMCASE - MAR Letak Rendah Tanpa FistelashyОценок пока нет
- NCP GDMДокумент5 страницNCP GDMShaina Millan100% (1)
- Unconventional Medicine Bonus ChapterДокумент63 страницыUnconventional Medicine Bonus ChapterDiana-Andreea AnghelОценок пока нет
- Diabetes Mellitus & Pregnancy: G.M PunarbawaДокумент27 страницDiabetes Mellitus & Pregnancy: G.M PunarbawaMartina RizkiОценок пока нет
- Gestational Diabetes Mellitus - NISALДокумент7 страницGestational Diabetes Mellitus - NISALKevin de SilvaОценок пока нет
- Diabetes MellitusДокумент29 страницDiabetes MellitusIMAFD67% (3)
- Fasting-Dm-Covid 14 March 2021 EditДокумент39 страницFasting-Dm-Covid 14 March 2021 EditrettiОценок пока нет
- Canadian Diabetes and Ramadan Fasting Position Statement RecommendationДокумент14 страницCanadian Diabetes and Ramadan Fasting Position Statement Recommendationsosmednya aristaОценок пока нет
- Diabetes Management During Ramadan May 2019Документ12 страницDiabetes Management During Ramadan May 2019توفيق البطرОценок пока нет
- Diabetes in Ramadan Aishah 1st AprilДокумент38 страницDiabetes in Ramadan Aishah 1st Aprilaliasmab87Оценок пока нет
- Atelier: Diabète Et Ramadan: Quels Sont Les Précautions À Prendre ?Документ14 страницAtelier: Diabète Et Ramadan: Quels Sont Les Précautions À Prendre ?Ekram HajjiОценок пока нет
- Komplikasi Akut Diabetes Selama BerpuasaДокумент18 страницKomplikasi Akut Diabetes Selama BerpuasaDewi Sri WulandariОценок пока нет
- Diabetes Mellitus: Anne Dawnay Biochemical MedicineДокумент26 страницDiabetes Mellitus: Anne Dawnay Biochemical MedicineJoni HermawanОценок пока нет
- RTD DM During RamadanДокумент33 страницыRTD DM During Ramadanakbar011512Оценок пока нет
- GDMДокумент30 страницGDMCharlz ZipaganОценок пока нет
- Appoach To Brittle Diabetes: Clinical Algorithm To Determine The EtiologyДокумент2 страницыAppoach To Brittle Diabetes: Clinical Algorithm To Determine The EtiologyMudassar SattarОценок пока нет
- NCMB316 Lec MidtermДокумент28 страницNCMB316 Lec Midterm2 - GUEVARRA, KYLE JOSHUA M.Оценок пока нет
- PCC HandbookДокумент193 страницыPCC HandbookMusa LandeОценок пока нет
- MNT Gestational Diabetes Dr. Shanthi Krishnasamy (RD)Документ28 страницMNT Gestational Diabetes Dr. Shanthi Krishnasamy (RD)Shanthi KrishnasamyОценок пока нет
- Diabetes and Ramadhan Practical Guide - Slide Deck - FINALДокумент68 страницDiabetes and Ramadhan Practical Guide - Slide Deck - FINALaliasmab87Оценок пока нет
- Diabetes MellitusДокумент7 страницDiabetes MellitusDrAlaa ZidanОценок пока нет
- Diabetes Mellitus 2021Документ61 страницаDiabetes Mellitus 2021Andarge ImperialОценок пока нет
- Diabetes Mellitus: NCM 116 Metabolism & Endocrine BSN 3Документ19 страницDiabetes Mellitus: NCM 116 Metabolism & Endocrine BSN 3Karen Kate AblesОценок пока нет
- Diabetes Mellitus: Medical Complications in PregnancyДокумент19 страницDiabetes Mellitus: Medical Complications in PregnancySenopati KhanjieОценок пока нет
- Neonatal HypoglycemiaДокумент1 страницаNeonatal HypoglycemiaYussika FernandaОценок пока нет
- Diabetes in PregnancyДокумент38 страницDiabetes in Pregnancybdzq3i12Оценок пока нет
- Diabetes Mellitus: Abdullah Al-Dahbali, Mpharm, PHDДокумент23 страницыDiabetes Mellitus: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيار100% (1)
- Presenter: Dr. P. Usha Rani Resident, ASRAMS, EluruДокумент60 страницPresenter: Dr. P. Usha Rani Resident, ASRAMS, EluruDivya Rekha KolliОценок пока нет
- Diabetes Mellitus Tipe 2Документ63 страницыDiabetes Mellitus Tipe 2HanaОценок пока нет
- Drugs For Diabetes PDFДокумент4 страницыDrugs For Diabetes PDFDylan RastoОценок пока нет
- Ginni Rani NewДокумент41 страницаGinni Rani NewEkta RajputОценок пока нет
- Endocrinology - 01 (2) - Diabetes (Courses in Therapeutics and Disease State Management)Документ62 страницыEndocrinology - 01 (2) - Diabetes (Courses in Therapeutics and Disease State Management)Ali AlyahawiОценок пока нет
- (Printing) Pass Medicine Notes - EndocrinologyДокумент73 страницы(Printing) Pass Medicine Notes - EndocrinologyJoanne HoОценок пока нет
- Diabetes MellitusДокумент27 страницDiabetes MellitusgibreilОценок пока нет
- Seminar 5 - DM in PregnancyДокумент19 страницSeminar 5 - DM in PregnancyHakimah K. SuhaimiОценок пока нет
- Diabetes and HypertensionДокумент6 страницDiabetes and HypertensionMary AgorillaОценок пока нет
- 03.BPJS 2023 Makbul Update Diabetes Management DiabetesДокумент36 страниц03.BPJS 2023 Makbul Update Diabetes Management DiabetesRini CanОценок пока нет
- Medical Disorders in PXДокумент49 страницMedical Disorders in PXSemon YohannesОценок пока нет
- (Endo) Diabetes, Obesity and Metabolic Syndrome - Dr. BermudezДокумент11 страниц(Endo) Diabetes, Obesity and Metabolic Syndrome - Dr. BermudezNoreen Hannah GabrielОценок пока нет
- CARBOHYDRATE METABOLISM AND DISORDERS (Herbal Med)Документ44 страницыCARBOHYDRATE METABOLISM AND DISORDERS (Herbal Med)AhjОценок пока нет
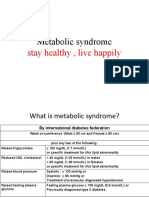
- Metabolic Syndrome: Stay Healthy, Live HappilyДокумент32 страницыMetabolic Syndrome: Stay Healthy, Live HappilykomalscientistОценок пока нет
- Diabetes Mellitus: (Assigned Report)Документ9 страницDiabetes Mellitus: (Assigned Report)regine maeОценок пока нет
- Diabetes Mellitus-2Документ15 страницDiabetes Mellitus-2Narmeen RahimОценок пока нет
- Diabetes Mellitus: MedicineДокумент4 страницыDiabetes Mellitus: MedicineKrista P. AguinaldoОценок пока нет
- Class 7 (26.07.2022)Документ53 страницыClass 7 (26.07.2022)Ãqûã FîggâОценок пока нет
- CR EndokrinДокумент14 страницCR EndokrinFajar SutrisnaОценок пока нет
- Prediabetes 1Документ21 страницаPrediabetes 1Nirmaa100% (2)
- 11.pregnancy & Diabetes MellitusДокумент23 страницы11.pregnancy & Diabetes Mellituskume senbetaОценок пока нет
- Diabetes - Mellitus - 1 - Y2 - 280915Документ24 страницыDiabetes - Mellitus - 1 - Y2 - 280915azizan hannyОценок пока нет
- PK - DR Toni - Metab Karbo Dan DMДокумент32 страницыPK - DR Toni - Metab Karbo Dan DMAyu DewiОценок пока нет
- Diabetes in PregnancyДокумент62 страницыDiabetes in Pregnancykapil khanalОценок пока нет
- NCM 116 Skills - Midterm NotesДокумент20 страницNCM 116 Skills - Midterm NotesmareginaОценок пока нет
- 6 Medical Disorders During PregnancyДокумент43 страницы6 Medical Disorders During PregnancyBethelAberaHaydamoОценок пока нет
- Topic Discussion DiabetsДокумент30 страницTopic Discussion Diabetsapi-538856946Оценок пока нет
- COvID Front Door v1.0Документ3 страницыCOvID Front Door v1.0Florin StanciuОценок пока нет
- ISTC-Pengobatan TB 2013Документ24 страницыISTC-Pengobatan TB 2013Muhammad mukramОценок пока нет
- Diabetes MellitusДокумент65 страницDiabetes MellitusOneTwoОценок пока нет
- Management of Diabetes Mellitus: Dr. Kartik Doshi 25.1.2012Документ80 страницManagement of Diabetes Mellitus: Dr. Kartik Doshi 25.1.2012Camille Honeyleith FernandoОценок пока нет
- International Journal of Surgery Open: Yophtahe Woldegerima Berhe, Amare Hailekiros Gebregzi, Nigussie Simeneh EndalewДокумент6 страницInternational Journal of Surgery Open: Yophtahe Woldegerima Berhe, Amare Hailekiros Gebregzi, Nigussie Simeneh EndalewfaeОценок пока нет
- Primal Testosterone EbookДокумент44 страницыPrimal Testosterone Ebook7nvzs8wn24Оценок пока нет
- Retrospective Characterization of Coma and Stupor in Dogs and Cats Presenting To A Multicenter Out-Of-Hours Service (2012-2015) : 386 AnimalsДокумент7 страницRetrospective Characterization of Coma and Stupor in Dogs and Cats Presenting To A Multicenter Out-Of-Hours Service (2012-2015) : 386 AnimalsLaura Pereira da SilvaОценок пока нет
- An Update Management of Acute Ischemic Stroke: SurotoДокумент36 страницAn Update Management of Acute Ischemic Stroke: SurotoShinta DianОценок пока нет
- Racial Differences in The Relationship of Glucose Concentrations and Hemoglobin A1cLevelsДокумент14 страницRacial Differences in The Relationship of Glucose Concentrations and Hemoglobin A1cLevelsRoberto López MataОценок пока нет
- Chandola SirДокумент118 страницChandola Sirpriyanka sharmaОценок пока нет
- VWA - Contemporary Management of Diabetes MellitusДокумент46 страницVWA - Contemporary Management of Diabetes MellitusVincenzina SoósОценок пока нет
- Sidiary: ManualДокумент133 страницыSidiary: ManualtomactinОценок пока нет
- Inclusive Household Disaster Preparedness WorkbookДокумент20 страницInclusive Household Disaster Preparedness WorkbookKatrina Coleen GaviolaОценок пока нет
- NCMB 316 Cu12 EndocrineДокумент84 страницыNCMB 316 Cu12 EndocrineJanine Dela CruzОценок пока нет
- Nutrition Through The Life Cycle 6th Edition Brown Test Bank 1Документ22 страницыNutrition Through The Life Cycle 6th Edition Brown Test Bank 1matthew100% (55)
- Measuring Blood Glucose LevelДокумент7 страницMeasuring Blood Glucose LevelHuda BehroozОценок пока нет
- LPL - PSC Rohini (Sector 8) D-11/148, GF SECTOR-8, ROHINI DelhiДокумент2 страницыLPL - PSC Rohini (Sector 8) D-11/148, GF SECTOR-8, ROHINI DelhiShivam Srivastava0% (1)
- Hyperosmolar Hyperglycemic StateДокумент10 страницHyperosmolar Hyperglycemic StateMirko S. León RguezОценок пока нет
- New Developments in Clinical Practice Guidelines: Invited CommunicationДокумент4 страницыNew Developments in Clinical Practice Guidelines: Invited CommunicationCar OrdzОценок пока нет
- Cozaar 25 MG: What Is Losartan (Cozaar) ?Документ25 страницCozaar 25 MG: What Is Losartan (Cozaar) ?nyzgirl17Оценок пока нет
- Review Notes For Diabetes MellitusДокумент8 страницReview Notes For Diabetes MellitusEditha LucasОценок пока нет
- Science (Reading For Meaning) - 1Документ68 страницScience (Reading For Meaning) - 1PeterОценок пока нет
- DiabetesДокумент2 страницыDiabetesKanika AnthonyОценок пока нет
- Emergency Drugs FileДокумент29 страницEmergency Drugs Filemmbire@gmail.comОценок пока нет
- Form2midyear ExamДокумент11 страницForm2midyear ExamBazilah HasanОценок пока нет
- 10 Evidence-Based Health Benefits of CinnamonДокумент15 страниц10 Evidence-Based Health Benefits of Cinnamonnic315Оценок пока нет