Вам также может понравиться
- Congenital Heart DiseaseДокумент77 страницCongenital Heart DiseaseMalueth Angui100% (1)
- Congenital Heart Disease - ASDДокумент36 страницCongenital Heart Disease - ASDAuni Akif Aleesa100% (1)
- Congenital Heart Disease - Cynotic AcynoticДокумент34 страницыCongenital Heart Disease - Cynotic Acynoticvruttika parmarОценок пока нет
- Nursing the NeonateОт EverandNursing the NeonateMaggie MeeksОценок пока нет
- Hemophilia in ChildrenДокумент16 страницHemophilia in ChildrenVinay Sahu100% (1)
- Ventricular Septal DefectДокумент55 страницVentricular Septal DefecthoneyworksОценок пока нет
- NeonatalresuscitationДокумент67 страницNeonatalresuscitationfidaОценок пока нет
- Transposition of Great ArteriesДокумент18 страницTransposition of Great Arteriesparmeshori100% (2)
- Neonatal SeizuresДокумент4 страницыNeonatal SeizuresSerag EdeenОценок пока нет
- Neonatal SeizuresДокумент13 страницNeonatal SeizuresLuis Daniel Bernal CondeОценок пока нет
- Brain DeathДокумент12 страницBrain DeathAbdallahMousaОценок пока нет
- Meconium Aspiration SyndromeДокумент7 страницMeconium Aspiration SyndromeAi Niech Inoel100% (1)
- Hepatitis in ChildrenДокумент2 страницыHepatitis in ChildrenShilpi SinghОценок пока нет
- Neonatal HypocalcemiaДокумент8 страницNeonatal HypocalcemiaCristina Fernández ValenciaОценок пока нет
- Neonatal Golden HourДокумент28 страницNeonatal Golden HourGendis Ayu ArdiasОценок пока нет
- Neonatal Sepsis LectureДокумент142 страницыNeonatal Sepsis Lectureokwadha simion0% (1)
- Transient Tachypnea of The Newborn (TTN)Документ6 страницTransient Tachypnea of The Newborn (TTN)Wivan Havilian DjohanОценок пока нет
- National Control of Dirrheal Diseases (CDD) Program ObjectivesДокумент6 страницNational Control of Dirrheal Diseases (CDD) Program ObjectivesJoy FucananОценок пока нет
- Pediatrics: by DR - Mohammad Z. Abu Sheikha@Документ101 страницаPediatrics: by DR - Mohammad Z. Abu Sheikha@صقر حوران100% (1)
- BSC Nursing: Medical Surgical Nursing Unit V - Disorders of The Cardio Vascular SystemДокумент34 страницыBSC Nursing: Medical Surgical Nursing Unit V - Disorders of The Cardio Vascular SystemPoova Ragavan100% (1)
- Rheumatic Fever and RHDДокумент49 страницRheumatic Fever and RHDbereket gashuОценок пока нет
- 05 Polycythemia in The NewbornДокумент11 страниц05 Polycythemia in The NewbornMorales Eli PediatraОценок пока нет
- Congenital SyphilisДокумент6 страницCongenital SyphilisFrozen Pandora MahayaОценок пока нет
- HypothermiaДокумент5 страницHypothermiaMRS CHAKRAPANIОценок пока нет
- Non Hodgkin Lymphoma in ChildrenДокумент4 страницыNon Hodgkin Lymphoma in ChildrenMilzan MurtadhaОценок пока нет
- Neonatal Hypoglycemia: 1.transient (Most Common) 2.persistenet (Less Common)Документ8 страницNeonatal Hypoglycemia: 1.transient (Most Common) 2.persistenet (Less Common)mohammadОценок пока нет
- Appproach To A Case of Status Epilepticus in PaediatricsДокумент45 страницAppproach To A Case of Status Epilepticus in PaediatricsChin NamОценок пока нет
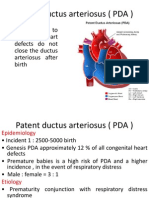
- Patent Ductus Arteriosus (PDA)Документ6 страницPatent Ductus Arteriosus (PDA)Sintia MardhaОценок пока нет
- Allergic Rhinitis in ChildrenДокумент7 страницAllergic Rhinitis in ChildrenTina MorleyОценок пока нет
- ALLERGIC RHINITIS IN CHILDREN RinaДокумент39 страницALLERGIC RHINITIS IN CHILDREN Rinarinajacky100% (2)
- Hematological Alterations: Disseminated Intravascular Coagulation (DIC)Документ16 страницHematological Alterations: Disseminated Intravascular Coagulation (DIC)jhommmmmОценок пока нет
- Persistent Newborn Pulmonary HypertensionДокумент10 страницPersistent Newborn Pulmonary HypertensionWali MoralesОценок пока нет
- Neonatal BLSДокумент18 страницNeonatal BLSPatrickNichols0% (1)
- Lec 2, Congenital Heart DiseasesДокумент61 страницаLec 2, Congenital Heart DiseasesAlexandrescuОценок пока нет
- Neonatal ExaminationДокумент50 страницNeonatal ExaminationCLEMENT50% (2)
- Approach To Bleeding NeonateДокумент20 страницApproach To Bleeding NeonateIndranil DuttaОценок пока нет
- Respiratory DistressДокумент11 страницRespiratory DistressHina MasoodОценок пока нет
- Hypoxic Ischemic EncephalopathyДокумент7 страницHypoxic Ischemic EncephalopathyJennesse May Guiao IbayОценок пока нет
- Congenital SyphilisДокумент3 страницыCongenital SyphilisadmusОценок пока нет
- Neonatal SepsisДокумент53 страницыNeonatal SepsisFrancis AmuzuОценок пока нет
- MECONIUM Aspiration SyndromeДокумент37 страницMECONIUM Aspiration SyndromekamalaОценок пока нет
- Idiopathic Thrombocytopenic PurpuraДокумент8 страницIdiopathic Thrombocytopenic PurpuraMonette Abalos MendovaОценок пока нет
- Renal Failure in ChildrenДокумент43 страницыRenal Failure in Childrendennyyy175Оценок пока нет
- AsphyxiaДокумент35 страницAsphyxiaAna Cristina Montillano100% (1)
- Newborn Respiratory Distress 11.28.2011Документ41 страницаNewborn Respiratory Distress 11.28.2011Emily EresumaОценок пока нет
- Hirschsprung DiseaseДокумент19 страницHirschsprung DiseaseUgi Rahul100% (1)
- DR Varsha Atul Shah Senior Consultant Dept of Neonatal and Devt Medicine, SGH Visiting Consultant Dept of Child Devt, KKHДокумент47 страницDR Varsha Atul Shah Senior Consultant Dept of Neonatal and Devt Medicine, SGH Visiting Consultant Dept of Child Devt, KKHJennifer MrjОценок пока нет
- Final Exam NotesДокумент24 страницыFinal Exam NotesNicholeGarcesCisnerosОценок пока нет
- OS 213 Pediatric AsthmaДокумент8 страницOS 213 Pediatric Asthma2012Оценок пока нет
- Laryngomalacia - PPTX Dr. FeriДокумент114 страницLaryngomalacia - PPTX Dr. FeriAldy BimaОценок пока нет
- Neonatal Seizures: Bhavith Ravi Medical StudentДокумент16 страницNeonatal Seizures: Bhavith Ravi Medical StudentkakuОценок пока нет
- Anatomic Disorders of Female Reproductive SystemДокумент42 страницыAnatomic Disorders of Female Reproductive SystemNelly AstikaОценок пока нет
- Atrial Septal Defect: by DR - AnandДокумент21 страницаAtrial Septal Defect: by DR - AnandJaya PrabhaОценок пока нет
- Status EpilepticusДокумент28 страницStatus EpilepticusDaniel AlfredОценок пока нет
- Pathophysiology of Birth AsphyxiaДокумент14 страницPathophysiology of Birth AsphyxiaEduardo Rios DuboisОценок пока нет
- A Neonate With Acute Kidney Injury: Case PresentationДокумент4 страницыA Neonate With Acute Kidney Injury: Case PresentationSahil DhamijaОценок пока нет
- Congenital Cyanotic Heart DiseaseДокумент26 страницCongenital Cyanotic Heart DiseaseAlokh Saha Raj100% (1)
- Etiology PPPДокумент24 страницыEtiology PPPCresty Estalilla100% (1)
- Perioperative Fluid Management in ChildrenДокумент31 страницаPerioperative Fluid Management in ChildrenRashmi SahaОценок пока нет
- Conginital Heart DiseaseДокумент19 страницConginital Heart DiseaseSanthosh.S.UОценок пока нет
- Soalan MEQ Head InjuryДокумент7 страницSoalan MEQ Head InjuryAuni Akif Aleesa100% (1)
- Table 2 of TMC501 Lesson 3 Go On Holiday (Prepared by Dr. Neo Kian Sen)Документ4 страницыTable 2 of TMC501 Lesson 3 Go On Holiday (Prepared by Dr. Neo Kian Sen)Auni Akif AleesaОценок пока нет
- Febrile FitДокумент3 страницыFebrile FitAuni Akif AleesaОценок пока нет
- Table 1 of TMC501 Lesson 2 Kampung Life (Prepared by Dr. Neo Kian Sen)Документ2 страницыTable 1 of TMC501 Lesson 2 Kampung Life (Prepared by Dr. Neo Kian Sen)Auni Akif AleesaОценок пока нет
- RainДокумент1 страницаRainAuni Akif Aleesa50% (2)
- Cell, TissueДокумент8 страницCell, TissueAuni Akif AleesaОценок пока нет
- Heart Failure - Nursing ManagementДокумент9 страницHeart Failure - Nursing ManagementAuni Akif Aleesa100% (1)
- Quick NOteДокумент7 страницQuick NOteAuni Akif Aleesa100% (1)
- Ebook Concepts of Fitness and Wellness A Comprehensive Lifestyle Approach 10Th Edition Corbin Test Bank Full Chapter PDFДокумент30 страницEbook Concepts of Fitness and Wellness A Comprehensive Lifestyle Approach 10Th Edition Corbin Test Bank Full Chapter PDFkaylinque98y2100% (11)
- April 2021 - Pediatric Emergency CareДокумент128 страницApril 2021 - Pediatric Emergency CareEdison Junior Juarez LaricoОценок пока нет
- Pathology of Blood VesselsДокумент80 страницPathology of Blood VesselsiqiqiqiqiqОценок пока нет
- Na Hypo PotomaniaДокумент7 страницNa Hypo Potomaniaanderson roberto oliveira de sousaОценок пока нет
- Physiology Mid Q Part 3 VIPДокумент16 страницPhysiology Mid Q Part 3 VIPDanah AlhusainiОценок пока нет
- Jalil 2017Документ24 страницыJalil 2017Karel ZertucheОценок пока нет
- Byrd PDFДокумент16 страницByrd PDFEghet SilviuОценок пока нет
- Uia 10 CARDIOVASCULAR PHYSIOLOGYДокумент7 страницUia 10 CARDIOVASCULAR PHYSIOLOGYLiliesther Erminda Hernandez VallecilloОценок пока нет
- Rendam Kaki Dengan Rebusan Jahe Merah Dapat Mencegah Terjadinya EklamsiaДокумент8 страницRendam Kaki Dengan Rebusan Jahe Merah Dapat Mencegah Terjadinya EklamsiaMellwandariskОценок пока нет
- Contemporary Outcomes of Percutaneous Closure of Patent Ductus Arteriosus in Adolescents and Adults PDFДокумент8 страницContemporary Outcomes of Percutaneous Closure of Patent Ductus Arteriosus in Adolescents and Adults PDFMuhammad IrfanОценок пока нет
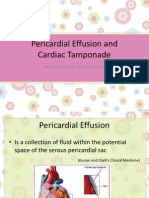
- Pericardial Effusion and Cardiac TamponadeДокумент18 страницPericardial Effusion and Cardiac TamponadeSiti Hamidah Abd Aziz100% (1)
- Basic ECG InterpretationДокумент16 страницBasic ECG InterpretationKim BadillesОценок пока нет
- Anatomy of Mitral ValveДокумент6 страницAnatomy of Mitral ValvesrhubanbabuОценок пока нет
- Fundamentals of CT PDFДокумент415 страницFundamentals of CT PDFAl Marchese100% (1)
- Antihypertensive DrugsДокумент62 страницыAntihypertensive DrugsYeshaa MiraniОценок пока нет
- Pacemaker Timing & IntervalsДокумент124 страницыPacemaker Timing & IntervalsNiranjan Reddy100% (1)
- 1 Tolerancia Al Esfuerzo MyersДокумент9 страниц1 Tolerancia Al Esfuerzo MyersAMALIAОценок пока нет
- Anph121lb CardiovascularДокумент28 страницAnph121lb CardiovascularDANIELA PEREZОценок пока нет
- Heart Failure: Christian Rey Cayabyab Y3 Medical Student University of LimerickДокумент16 страницHeart Failure: Christian Rey Cayabyab Y3 Medical Student University of LimerickChristian CayabyabОценок пока нет
- Carto3 Fact SheetДокумент3 страницыCarto3 Fact SheetVimal NishadОценок пока нет
- Guidelines and Standards: KeywordsДокумент18 страницGuidelines and Standards: KeywordsTuan HaiОценок пока нет
- ACC-AHA Guidelines Heart FailureДокумент56 страницACC-AHA Guidelines Heart FailureUswatul HasanahОценок пока нет
- Diagnosis and Management of Myocardial InfarctionДокумент69 страницDiagnosis and Management of Myocardial InfarctionSanjana GkОценок пока нет
- Ananya Basu Internal Medicine Clinical CaseДокумент4 страницыAnanya Basu Internal Medicine Clinical Caseavnikasharma4889Оценок пока нет
- 2018CV03Документ22 страницы2018CV03Cheng-Ting WuОценок пока нет
- Divine Intervention Step 2CK Podcasts Notes - Read Only File - Docx (Dragged) 4Документ3 страницыDivine Intervention Step 2CK Podcasts Notes - Read Only File - Docx (Dragged) 4winston1234Оценок пока нет
- Circulatory SystemДокумент21 страницаCirculatory SystemKumar Sujeet100% (1)
- Regulation of Coronary Blood Flow PDFДокумент330 страницRegulation of Coronary Blood Flow PDFAlin-Octavian BorinaОценок пока нет
- The Transport System IB Qq'sДокумент12 страницThe Transport System IB Qq'sJohn OsborneОценок пока нет
- Unicare Product List (Oct. 2023)Документ3 страницыUnicare Product List (Oct. 2023)rizaie.azizuddin2022Оценок пока нет