Вам также может понравиться
- Microscopic Examination of UrineДокумент4 страницыMicroscopic Examination of UrineGlaiza Erika Baes GudaОценок пока нет
- Practical Manual for Detection of Parasites in Feces, Blood and Urine SamplesОт EverandPractical Manual for Detection of Parasites in Feces, Blood and Urine SamplesОценок пока нет
- Urinalysis and Body Fluids2020Документ47 страницUrinalysis and Body Fluids2020MONFOLA100% (1)
- AUB - Microscopic Analysis of UrineДокумент4 страницыAUB - Microscopic Analysis of UrineJeanne Rodiño100% (1)
- AUB - Physical Examination of UrineДокумент3 страницыAUB - Physical Examination of UrineJeanne RodiñoОценок пока нет
- Non Protein CompoundsДокумент64 страницыNon Protein CompoundsAbigail Mayled LausОценок пока нет
- AUB - Urine Screening For Metabolic DisordersДокумент3 страницыAUB - Urine Screening For Metabolic DisordersJeanne Rodiño100% (1)
- Relevance of Serum Tumor MarkersДокумент25 страницRelevance of Serum Tumor MarkersDrPawan KirtaniОценок пока нет
- Analysis of Physical Properties of UrineДокумент2 страницыAnalysis of Physical Properties of UrineameerabestОценок пока нет
- Bacte TestДокумент10 страницBacte TestRiondalionОценок пока нет
- Physical Examination of UrineДокумент4 страницыPhysical Examination of UrineIceОценок пока нет
- Principles of Clinical Chemistry AutomationДокумент25 страницPrinciples of Clinical Chemistry AutomationChristine Rodriguez-Guerrero50% (2)
- Blood Bank IДокумент136 страницBlood Bank IPerlie CОценок пока нет
- Clearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSДокумент25 страницClearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSChandan SahОценок пока нет
- 3 Chemical Examination of UrineДокумент82 страницы3 Chemical Examination of UrineJake Real Dela RocaОценок пока нет
- Specimen Collection and Processing For Hemostasis TestingДокумент22 страницыSpecimen Collection and Processing For Hemostasis TestingTom Anthony Tonguia100% (1)
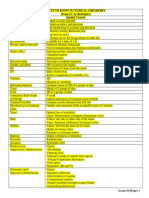
- MUST To KNOW in Clinical ChemistryДокумент53 страницыMUST To KNOW in Clinical ChemistryTristan Jay CalabiaОценок пока нет
- 3 Concentration Techniques SedimentationДокумент18 страниц3 Concentration Techniques SedimentationFatihah JahsmiОценок пока нет
- Chapter 14 - Routine and Point of Care Testing in HematologyДокумент10 страницChapter 14 - Routine and Point of Care Testing in HematologyNathaniel Sim100% (1)
- M6 Histopath ImpregantionAndEmbeddingДокумент4 страницыM6 Histopath ImpregantionAndEmbeddingninaОценок пока нет
- Coagulation NotesДокумент14 страницCoagulation NotesthrowawyОценок пока нет
- 3-1 Bacterial Identification TechniquesДокумент64 страницы3-1 Bacterial Identification TechniquesSri Wahyunie100% (1)
- Prepartion of Blood Smear Hematology PresentationДокумент44 страницыPrepartion of Blood Smear Hematology PresentationArslan ArshadОценок пока нет
- COMPLETE BLOOD COUNT Lecture GuideДокумент9 страницCOMPLETE BLOOD COUNT Lecture GuideKaycee Gretz LorescaОценок пока нет
- Medical Parasitology - FullДокумент30 страницMedical Parasitology - FullJesse Osborn100% (2)
- Section 13 - Hematology (Updated)Документ34 страницыSection 13 - Hematology (Updated)Lorelie CarlosОценок пока нет
- Urine Specimen Collection: Ms. Sneha SehrawatДокумент36 страницUrine Specimen Collection: Ms. Sneha SehrawatRajaОценок пока нет
- Lesson 22 PDFДокумент5 страницLesson 22 PDFfaeОценок пока нет
- Coagulation TestsДокумент25 страницCoagulation Testsdave_1128Оценок пока нет
- Aubf Lec (2 Week) Physical Examination of Urine: Color, Clarity Specific GravityДокумент38 страницAubf Lec (2 Week) Physical Examination of Urine: Color, Clarity Specific GravityAngela ReyesОценок пока нет
- CM Stool Examination (Ocfemia, Eliazel Galorio - BSLABSCI-PLTCIДокумент30 страницCM Stool Examination (Ocfemia, Eliazel Galorio - BSLABSCI-PLTCIeliazel ocfemiaОценок пока нет
- Board Exam Topic ChecklistДокумент3 страницыBoard Exam Topic ChecklistVianney Angeli LorenzanaОценок пока нет
- Blood Group Systems ISBTДокумент25 страницBlood Group Systems ISBTkusumahpratiwi100% (1)
- Laboratory Diagnosis of InfectionДокумент4 страницыLaboratory Diagnosis of InfectionHairul Anuar100% (1)
- Standard Operating Procedure: Biosystems Ba400Документ5 страницStandard Operating Procedure: Biosystems Ba400Mohamad QinaoiОценок пока нет
- Hematology 2 Topic 2 Prelim2222Документ73 страницыHematology 2 Topic 2 Prelim2222Mary Lyka ReyesОценок пока нет
- Gel TechnologyДокумент2 страницыGel TechnologyJai Carungay100% (1)
- A. B. C. A. B. C. D.: Clinical Chemistry II - Prelims (Bandala)Документ19 страницA. B. C. A. B. C. D.: Clinical Chemistry II - Prelims (Bandala)IceОценок пока нет
- Practical Hematology Manual #1Документ48 страницPractical Hematology Manual #1walhaliОценок пока нет
- Urinalysis and Body Fluid CollectionsДокумент48 страницUrinalysis and Body Fluid CollectionsladydianamacОценок пока нет
- Eprubete. Culori. UtilizareДокумент3 страницыEprubete. Culori. UtilizareCuCUОценок пока нет
- Basic Clinical Chemistry TestsДокумент49 страницBasic Clinical Chemistry TestsMegbaru100% (1)
- General Urine Examination (Urinalysis)Документ24 страницыGeneral Urine Examination (Urinalysis)Ali RonaldoОценок пока нет
- ENZYMOLOGYДокумент2 страницыENZYMOLOGYCarla Lagar FloresОценок пока нет
- Morphology OF Red Blood CellsДокумент36 страницMorphology OF Red Blood CellsFrancis ValdezОценок пока нет
- c4000 Stand Alone Specifications PDFДокумент6 страницc4000 Stand Alone Specifications PDFRuben DuranОценок пока нет
- Chapter 15 - Examination of The Peripheral Blood Film and Correlation With The Complete Blood CountДокумент7 страницChapter 15 - Examination of The Peripheral Blood Film and Correlation With The Complete Blood CountNathaniel SimОценок пока нет
- Intro To Urinalysis & Physical ExamДокумент62 страницыIntro To Urinalysis & Physical ExamRod PasionОценок пока нет
- Typhidot TestДокумент3 страницыTyphidot TestHisyam IshakОценок пока нет
- Chapter 4 Physical Examination PDFДокумент4 страницыChapter 4 Physical Examination PDFJulie Anne Soro ValdezОценок пока нет
- Blood Smear Examination 1معدل Документ74 страницыBlood Smear Examination 1معدل Kenesa100% (1)
- Examination of Specimens For ParasitesДокумент32 страницыExamination of Specimens For ParasitesJhost Clinton PurbaОценок пока нет
- A Case Study On Urinalysis and Body FluidsДокумент17 страницA Case Study On Urinalysis and Body Fluidsrakish16Оценок пока нет
- Pre-Analytical Consideration and Venipuncture ComplicationsДокумент52 страницыPre-Analytical Consideration and Venipuncture ComplicationsVenom100% (1)
- Exercise 1: Tools in The Laboratory: 1. AutoclaveДокумент48 страницExercise 1: Tools in The Laboratory: 1. AutoclaverayaimОценок пока нет
- Stool Analysis and Other Body Fluid AnalysisДокумент51 страницаStool Analysis and Other Body Fluid AnalysisPutri Senna Rahayu100% (2)
- Urine AnalysisДокумент69 страницUrine AnalysisAffan ElahiОценок пока нет
- Microbiology - ParasitologyДокумент34 страницыMicrobiology - ParasitologySasi DharanОценок пока нет
- Glucocorticoids in Systemic Lupus Erythematosus. Ten Questions and Some IssuesДокумент13 страницGlucocorticoids in Systemic Lupus Erythematosus. Ten Questions and Some IssuesSundas EjazОценок пока нет
- q8 Wellness PlanДокумент3 страницыq8 Wellness PlanabstabsОценок пока нет
- LA Union: PDRRM OДокумент32 страницыLA Union: PDRRM OEnash RidОценок пока нет
- Methodology and Project Design 4Документ4 страницыMethodology and Project Design 4api-706947027Оценок пока нет
- Image FilesДокумент264 страницыImage FilesSoksatya Korsal100% (1)
- Dental EssayДокумент3 страницыDental Essayvaleriana calaniОценок пока нет
- Homicide Disguised by SuicideДокумент3 страницыHomicide Disguised by SuicideMarlene Gonzalez FcoОценок пока нет
- 10th Monthly Compliance Report On Parkland Memorial HospitalДокумент92 страницы10th Monthly Compliance Report On Parkland Memorial HospitalmilesmoffeitОценок пока нет
- Broward Medical Examiner ReportДокумент42 страницыBroward Medical Examiner ReportrabdillОценок пока нет
- Uterine Prolapse in A Primigravid Woman JournalДокумент13 страницUterine Prolapse in A Primigravid Woman JournalFadhlyanyОценок пока нет
- Acutrak2 Radial Head Case StudyДокумент2 страницыAcutrak2 Radial Head Case StudyDinesh KumarОценок пока нет
- CSF Catalogue enДокумент76 страницCSF Catalogue enHarshitShuklaОценок пока нет
- Adaptive Immunity: Yanne Pradwi EfendiДокумент25 страницAdaptive Immunity: Yanne Pradwi EfendiMelissa Indah SariОценок пока нет
- 65 Interview Questions For Nurses.13Документ3 страницы65 Interview Questions For Nurses.13natalieshirleyОценок пока нет
- Cycle BeadsДокумент2 страницыCycle Beadsgihan200100% (2)
- Selective Awareness TherapyДокумент10 страницSelective Awareness TherapyHashem Al AttasОценок пока нет
- Preterm Labour: Muhammad Hanif Final Year MBBSДокумент32 страницыPreterm Labour: Muhammad Hanif Final Year MBBSArslan HassanОценок пока нет
- Nerium OleanderДокумент20 страницNerium OleanderGeneizzel GotuatoОценок пока нет
- Congenital Adrenal HyperplasiaДокумент30 страницCongenital Adrenal HyperplasiaIrene Jordan100% (1)
- NCP PediaДокумент2 страницыNCP PediaAdrian John DecolongonОценок пока нет
- Unit 1 Chap 1 and 2Документ7 страницUnit 1 Chap 1 and 2Ariane Grace OcampoОценок пока нет
- Paracetamol Overdose Treatment NomogramДокумент1 страницаParacetamol Overdose Treatment NomogramCoenraad van SchoorОценок пока нет
- Artsanto R, Doso Sutiyono, Witjaksono : Bagian Anestesiologi Dan Terapi Intensif FK Undip/ RSUP Dr. Kariadi, SemarangДокумент12 страницArtsanto R, Doso Sutiyono, Witjaksono : Bagian Anestesiologi Dan Terapi Intensif FK Undip/ RSUP Dr. Kariadi, SemarangAdhyОценок пока нет
- Hospital ThesisДокумент47 страницHospital ThesisninsОценок пока нет
- Praposal DM-1Документ117 страницPraposal DM-1sanjay sabdeОценок пока нет
- Topical Steroids DermatologyДокумент23 страницыTopical Steroids DermatologyRitika Agarwal100% (1)
- Paper-Organ DonationДокумент7 страницPaper-Organ Donationapi-400417633Оценок пока нет
- Meyer Et Al 2001Документ38 страницMeyer Et Al 2001MIAОценок пока нет
- Institute of Nursing: Far Eastern UniversityДокумент3 страницыInstitute of Nursing: Far Eastern UniversityaleccespirituОценок пока нет
- Psychiatry 136 Q&AДокумент37 страницPsychiatry 136 Q&AManushi HenadeeraОценок пока нет