Вам также может понравиться
- Akita SavvyДокумент170 страницAkita Savvylinbillion99386% (7)
- snc2d Biology Unit TestДокумент6 страницsnc2d Biology Unit Testapi-3078129790% (3)
- MSE - Bipolar (Manic Phase)Документ3 страницыMSE - Bipolar (Manic Phase)Carla Tongson MaravillaОценок пока нет
- Dear Abby Unit 4 EndДокумент11 страницDear Abby Unit 4 EndBeatriz AckermannОценок пока нет
- Sandeep Sharma Deepa Rawat Sandeep Sharma, Deep RawatДокумент29 страницSandeep Sharma Deepa Rawat Sandeep Sharma, Deep RawatAngelica PingulОценок пока нет
- Msds HCL 0,1 NДокумент6 страницMsds HCL 0,1 NRinie Aeryn Nayndine'netzzОценок пока нет
- Studies of Drug Induced Birth DefectsДокумент16 страницStudies of Drug Induced Birth DefectsArvind Nag100% (1)
- Paranoid SchizophreniaДокумент26 страницParanoid SchizophreniaCrisha Ann Billones BacutaОценок пока нет
- Generalized Anxiety DisorderДокумент8 страницGeneralized Anxiety DisorderTanvi SharmaОценок пока нет
- CasestudyДокумент6 страницCasestudyapi-297258832Оценок пока нет
- Dissociative Identity DisorderДокумент4 страницыDissociative Identity DisorderalfredОценок пока нет
- Madeleine Leininger: Culture Care Diversity and Universality TheoryДокумент23 страницыMadeleine Leininger: Culture Care Diversity and Universality TheoryMark Torres AguilarОценок пока нет
- Mental Status Examination FormДокумент8 страницMental Status Examination FormSheena VallesОценок пока нет
- Case Study - Personality Disorders: College of Nursing Psychiatric NursingДокумент2 страницыCase Study - Personality Disorders: College of Nursing Psychiatric NursingCamille SindayОценок пока нет
- Psych Case StudyДокумент32 страницыPsych Case StudyAndrea Isabel U. O'DellОценок пока нет
- Bipolar NCPДокумент2 страницыBipolar NCPBrenn Marie RamosОценок пока нет
- Nursing Interventions in SchizophreniaДокумент24 страницыNursing Interventions in SchizophreniaChristian Apelo Serquillos0% (1)
- The Mental Status ExamДокумент7 страницThe Mental Status ExamAnonymous ewPKlLWtfhОценок пока нет
- OlanzapineДокумент3 страницыOlanzapineLeris Luigi VictorioОценок пока нет
- Group NCPДокумент17 страницGroup NCPNiña Noreen Torres VallegaОценок пока нет
- Bachelor of Science in Nursing: Intensive Nursing Practicum: Rle LCP Module Rle LCP Unit WeekДокумент8 страницBachelor of Science in Nursing: Intensive Nursing Practicum: Rle LCP Module Rle LCP Unit WeekMichelle Gliselle Guinto MallareОценок пока нет
- The Mini Mental Status ExaminationДокумент4 страницыThe Mini Mental Status ExaminationAssignmentLab.comОценок пока нет
- Introduction-: Post Traumatic Stress Disorder (PTSD)Документ10 страницIntroduction-: Post Traumatic Stress Disorder (PTSD)preeti sharmaОценок пока нет
- Ethical Schools of Thought - Part TwoДокумент56 страницEthical Schools of Thought - Part TwoFille_Anne_Lay_1019100% (1)
- CHAPTER 16 - Schizophrenia 2Документ15 страницCHAPTER 16 - Schizophrenia 2RebeccaОценок пока нет
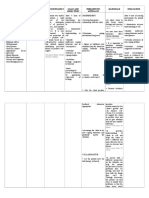
- Nursing Care Plan Nursing Diagnosis Goals/ Objectives Interventions EvaluationДокумент1 страницаNursing Care Plan Nursing Diagnosis Goals/ Objectives Interventions EvaluationRichard BaigОценок пока нет
- Mental Status ExamДокумент11 страницMental Status ExamShanette Mckinney100% (1)
- Nursing Care Plan: NCM 109 Rle Clinical Wednesday 7:00 AM - 12:00 PMДокумент10 страницNursing Care Plan: NCM 109 Rle Clinical Wednesday 7:00 AM - 12:00 PMBiway RegalaОценок пока нет
- Case Study - Mental Status ExaminationДокумент5 страницCase Study - Mental Status ExaminationSrivathsanОценок пока нет
- NCMH Case Study 2Документ22 страницыNCMH Case Study 2Kristoff StJohn Gamilla CuasayОценок пока нет
- NPI Feb2,7 And8Документ14 страницNPI Feb2,7 And8Mikko Anthony Pingol AlarconОценок пока нет
- 13 Areas of Assessment 1 6 RevisedДокумент10 страниц13 Areas of Assessment 1 6 RevisedSherena NicolasОценок пока нет
- NCP001 IsolationДокумент2 страницыNCP001 IsolationJoyh LasutaОценок пока нет
- Care of Patients With Maladaptive Patterns of Behavior: Psychiatric Mental Health Nursing 8 Edition Sheila VidebeckДокумент45 страницCare of Patients With Maladaptive Patterns of Behavior: Psychiatric Mental Health Nursing 8 Edition Sheila VidebeckGrape JuiceОценок пока нет
- Nurse Patient ShipДокумент97 страницNurse Patient Shipcharby12108272100% (2)
- Psychotropic DrugsДокумент2 страницыPsychotropic DrugsMj BrionesОценок пока нет
- Shutter Island Movie AnalysisДокумент3 страницыShutter Island Movie AnalysisBrian Lee Martin GonzalesОценок пока нет
- Spinal Cord InjuryДокумент28 страницSpinal Cord InjuryLouie John AbilaОценок пока нет
- 5 Three Mental OperationsДокумент12 страниц5 Three Mental OperationsSherwin Pazzibugan100% (1)
- Nursing Care Plan (NCP) For SchizophreniformДокумент8 страницNursing Care Plan (NCP) For SchizophreniformRisa Sol AriasОценок пока нет
- Process RecordingДокумент6 страницProcess RecordingteuuuuОценок пока нет
- Dissociative Identity Disorder Psycho PathologyДокумент1 страницаDissociative Identity Disorder Psycho PathologyfridurtОценок пока нет
- Anorexia Nervosa - Bulimia NervosaДокумент17 страницAnorexia Nervosa - Bulimia Nervosaapi-37642150% (1)
- NCPДокумент4 страницыNCPJoseph Dableo ParreñoОценок пока нет
- NCP Psych RotationДокумент3 страницыNCP Psych RotationFrancis Alfred EscaranОценок пока нет
- Psychiatric Nursing - Mental Status ExaminationДокумент4 страницыPsychiatric Nursing - Mental Status ExaminationChien Lai R. BontuyanОценок пока нет
- Analysis of The Nurse Manager RoleДокумент8 страницAnalysis of The Nurse Manager Roleapi-239630424Оценок пока нет
- Nursing Prioritization (Schizophrenia)Документ6 страницNursing Prioritization (Schizophrenia)Elaine Dionisio TanОценок пока нет
- MseДокумент5 страницMseYnaffit Alteza UntalОценок пока нет
- PSYCH Defensive CopingДокумент3 страницыPSYCH Defensive CopingJvWoodzОценок пока нет
- MseДокумент11 страницMseClyde R.OrtegaОценок пока нет
- Transcultural Perspective in Nursing Care For Children PDFДокумент41 страницаTranscultural Perspective in Nursing Care For Children PDFJade CatubayОценок пока нет
- Case StudyДокумент13 страницCase Studyapi-508178512Оценок пока нет
- Preliterate Times The Medieval Period: Era of Magico - Religious Explanation Era of AlienationДокумент6 страницPreliterate Times The Medieval Period: Era of Magico - Religious Explanation Era of AlienationJezreel Joyce RufiñoОценок пока нет
- Chapter 6 Somatic-Symptom-and-Related-Disorders-and-Dissociative-DisordersДокумент3 страницыChapter 6 Somatic-Symptom-and-Related-Disorders-and-Dissociative-DisordersAnnie SumacotОценок пока нет
- Schizophrenia PDFДокумент32 страницыSchizophrenia PDFJoyVee Pillagara-De LeonОценок пока нет
- Counselling LetterДокумент1 страницаCounselling LetterSeann LorescoОценок пока нет
- MSEДокумент20 страницMSEJenny YenОценок пока нет
- Process RecordingДокумент9 страницProcess Recordingnailed_heartОценок пока нет
- Mental Health AssessmentДокумент1 страницаMental Health AssessmentyasminОценок пока нет
- Abnormal Psychology: Introduction To PsychopathologyДокумент5 страницAbnormal Psychology: Introduction To PsychopathologyYanaKarununganОценок пока нет
- SchizophreniaДокумент9 страницSchizophreniaQueen Bee (Tt)Оценок пока нет
- DARUNDAY - NCM 117 Asynchronous ActivityДокумент17 страницDARUNDAY - NCM 117 Asynchronous ActivityEzra Miguel DarundayОценок пока нет
- Abnormal Psychology: Learning OutcomesДокумент31 страницаAbnormal Psychology: Learning OutcomesAlejandro MoralesОценок пока нет
- How To Approach Psychotic Symptoms in A Non-Specialist SettingДокумент6 страницHow To Approach Psychotic Symptoms in A Non-Specialist SettingNicholasОценок пока нет
- Rescue AsdДокумент17 страницRescue Asdaloisiaa8Оценок пока нет
- 0610 s12 QP 33Документ24 страницы0610 s12 QP 33karan79Оценок пока нет
- Blg1501 May June 2011 - Memorandum-1Документ4 страницыBlg1501 May June 2011 - Memorandum-1Janine Toffar100% (1)
- Diagnóstico TrombofiliaДокумент87 страницDiagnóstico TrombofiliaEugenio Torres100% (1)
- Prenatal DevelopmentДокумент33 страницыPrenatal DevelopmentDexter Nario0% (1)
- Fallout TTRPG v2.0 PDFДокумент179 страницFallout TTRPG v2.0 PDFJavontay PeoplesОценок пока нет
- 7B ReproductionДокумент31 страница7B ReproductionPerry Sin50% (2)
- Natural History of HIV Infection by DR A K Gupta, Addl. Project Director, DSACSДокумент29 страницNatural History of HIV Infection by DR A K Gupta, Addl. Project Director, DSACSdr.a.k.gupta6924100% (3)
- Usmle QДокумент46 страницUsmle QRoh Jiten100% (1)
- Muscular SystemДокумент8 страницMuscular Systemtheodore_estradaОценок пока нет
- Bone DensitometryДокумент42 страницыBone DensitometryWira Dat100% (1)
- Abdi Et Al. 2008Документ6 страницAbdi Et Al. 2008argos1301Оценок пока нет
- Antigen Assignment Final File PDFДокумент14 страницAntigen Assignment Final File PDFAbdul RafayОценок пока нет
- Biotechnology and The Human GoodДокумент225 страницBiotechnology and The Human GoodIvan Castillo Dcv100% (1)
- PCRДокумент31 страницаPCRsrgОценок пока нет
- Laporan Asuhan Keperawatan Bahasa InggrisДокумент8 страницLaporan Asuhan Keperawatan Bahasa InggrisBagus Wijanarko100% (1)
- ST Pauls Freedom NewsletterДокумент12 страницST Pauls Freedom Newsletterapi-247685481Оценок пока нет
- Chap 3 Paper - Theoretical Frameworks and Nursing ResearchДокумент9 страницChap 3 Paper - Theoretical Frameworks and Nursing ResearchEtty EriyantiОценок пока нет
- Neutrophil EbookДокумент468 страницNeutrophil EbookNathália LuísaОценок пока нет
- Congenital and Hereditary Diseases Introduction-1Документ21 страницаCongenital and Hereditary Diseases Introduction-1Melvin OnyanchaОценок пока нет
- Mgs Syllabus ZOOLOGY PDFДокумент32 страницыMgs Syllabus ZOOLOGY PDFhsjsjОценок пока нет
- Body Cavities PPT & Anatomical SystemДокумент10 страницBody Cavities PPT & Anatomical Systemnandhini raguОценок пока нет
- Bacterial Diseases Rice 2015Документ13 страницBacterial Diseases Rice 2015Teguh PratamaОценок пока нет
- Metabolic EngineeringДокумент9 страницMetabolic EngineeringArup ChakrabortyОценок пока нет
- Important Definitions: Nervous SystemДокумент4 страницыImportant Definitions: Nervous SystemValeri LopezОценок пока нет