Вам также может понравиться
- Developmental Dysplasia of The Hip: Muhammad Rizal, DR., SpotДокумент36 страницDevelopmental Dysplasia of The Hip: Muhammad Rizal, DR., Spotshintadevii100% (1)
- Edu - DDH Final 19.5.07Документ27 страницEdu - DDH Final 19.5.07Premnivas ParasuramanОценок пока нет
- Developmental Dysplasia of The HipДокумент30 страницDevelopmental Dysplasia of The HipJefry SОценок пока нет
- Ultrasound Hip DysplasiaДокумент42 страницыUltrasound Hip DysplasiaolegОценок пока нет
- CDH Treatment GuideДокумент50 страницCDH Treatment GuideCut Riska NovizaОценок пока нет
- Developmental Dysplasia of Hip (DDHДокумент50 страницDevelopmental Dysplasia of Hip (DDHNarishaAmeliaОценок пока нет
- Developmental Hip Dysplasia Diagnosis and TreatmentДокумент12 страницDevelopmental Hip Dysplasia Diagnosis and TreatmentFifi Chi Keluarga PrajaОценок пока нет
- DDHДокумент30 страницDDHsayedmОценок пока нет
- 3.pediatric Hip DisordersДокумент92 страницы3.pediatric Hip DisordersMahmoud Abu Al AmrainОценок пока нет
- Developmental Hip Dysplasia and DislocationДокумент51 страницаDevelopmental Hip Dysplasia and Dislocationandi firdha restuwatiОценок пока нет
- DDH Treatment - PFДокумент30 страницDDH Treatment - PFHendra SantosoОценок пока нет
- Developmental Dysplasia of Hip (DDH) : Nizar Abdul MajeedДокумент37 страницDevelopmental Dysplasia of Hip (DDH) : Nizar Abdul MajeedAh ZhangОценок пока нет
- Development Dysplasia of The Hip-2Документ107 страницDevelopment Dysplasia of The Hip-2Dr. Vishal singhОценок пока нет
- Developmental Dysplasia of The HipДокумент86 страницDevelopmental Dysplasia of The Hipadekunle ajayiОценок пока нет
- Hip ProblemsДокумент46 страницHip ProblemsDhiya' VinaОценок пока нет
- Overview Congenital Musculoskeletal DisorderДокумент84 страницыOverview Congenital Musculoskeletal DisorderRyan Trian100% (3)
- Developmental Dysplasia of the Hip (DDH) GuideДокумент126 страницDevelopmental Dysplasia of the Hip (DDH) GuideSameh AbdelaalОценок пока нет
- Developmental Dysplasia of The HipДокумент72 страницыDevelopmental Dysplasia of The HipVignesh WaranОценок пока нет
- Development Dysplasia of HipДокумент151 страницаDevelopment Dysplasia of HipKyla Obrien100% (1)
- Developmental Dysplasia of The HipДокумент33 страницыDevelopmental Dysplasia of The HipJoy KirumbaОценок пока нет
- DDH Developmental Hip DysplasiaДокумент67 страницDDH Developmental Hip DysplasiaGladys MainaОценок пока нет
- Congenital Dislocation of HipДокумент18 страницCongenital Dislocation of HipBikash DhitalОценок пока нет
- Vaginal Breech DeliveryДокумент33 страницыVaginal Breech DeliveryTriani Dwi NingsihОценок пока нет
- Preterm BreechДокумент38 страницPreterm Breechorin78Оценок пока нет
- DDHДокумент38 страницDDHSanjiv GoyalОценок пока нет
- DDHДокумент174 страницыDDHVikas RaiОценок пока нет
- DislocationДокумент29 страницDislocationtsega tilahunОценок пока нет
- Paediatric Orthopaedic Conditions GuideДокумент73 страницыPaediatric Orthopaedic Conditions GuideMuhamad Agung SupriyantoОценок пока нет
- Dr. Robert Tirtowijoyo (Paediatric Condition) Inggris UMJ Maret 2008 EditedДокумент73 страницыDr. Robert Tirtowijoyo (Paediatric Condition) Inggris UMJ Maret 2008 EditedMuhamad Agung SupriyantoОценок пока нет
- Newborn ExaminationДокумент45 страницNewborn ExaminationHamka HamОценок пока нет
- ObstetricsДокумент34 страницыObstetricshassanwejdan1Оценок пока нет
- Fetal Growth RestrictionДокумент56 страницFetal Growth RestrictionKanika VermaОценок пока нет
- OME Peds NotesДокумент11 страницOME Peds Notessmian08Оценок пока нет
- IUGR Diagnosis and Management GuideДокумент43 страницыIUGR Diagnosis and Management GuideAzura MotovlogОценок пока нет
- CongenitalДокумент43 страницыCongenitalxantheОценок пока нет
- TRUMAДокумент56 страницTRUMAzainabd1964Оценок пока нет
- IHDI Ortho Presentation WebДокумент7 страницIHDI Ortho Presentation WebC Martin TraumatoОценок пока нет
- Visual Diagnosis and Dysmorphology Series: Trisomy 21 Approach and ManagementДокумент21 страницаVisual Diagnosis and Dysmorphology Series: Trisomy 21 Approach and ManagementisauraОценок пока нет
- Breech Presentation 2020Документ73 страницыBreech Presentation 2020Max ZealОценок пока нет
- Developmental Dysplasia of The HipДокумент33 страницыDevelopmental Dysplasia of The HipQasem Rababah100% (1)
- Pathologies of The HipДокумент57 страницPathologies of The HipFreeburn SimunchembuОценок пока нет
- Understanding Contracted PelvisДокумент37 страницUnderstanding Contracted PelvisSona shaji100% (3)
- Menejemen Fisioterapi - Conginetal Hip DislocationДокумент79 страницMenejemen Fisioterapi - Conginetal Hip DislocationMufidah AlhadarОценок пока нет
- Common Pediatric Disorders of The Lower Extremity Affecting GaitДокумент90 страницCommon Pediatric Disorders of The Lower Extremity Affecting Gaithard3336Оценок пока нет
- SLIDE Scoliosis SRSДокумент48 страницSLIDE Scoliosis SRSAnonymous x2OJJmi9Z100% (2)
- Aleppo Capital of Islamic Culture 2006Документ62 страницыAleppo Capital of Islamic Culture 2006A Mounhem ObaideenОценок пока нет
- 28 - Fetal Growth DisordersДокумент44 страницы28 - Fetal Growth DisordersAbdelrahman ElsaadawiОценок пока нет
- Amenorrheamadeeasyslideshare 2015 150423165553 Conversion Gate01 PDFДокумент51 страницаAmenorrheamadeeasyslideshare 2015 150423165553 Conversion Gate01 PDFHerman FiraОценок пока нет
- 3 Problems With The Passenger and Powers of LaborДокумент105 страниц3 Problems With The Passenger and Powers of LaborRaquel M. MendozaОценок пока нет
- Genu Varum and Genu Valgum Causes DiagnosisДокумент33 страницыGenu Varum and Genu Valgum Causes DiagnosisIstianah Es100% (1)
- MRCPCH - Renal ImagingДокумент28 страницMRCPCH - Renal ImagingarjumandОценок пока нет
- CPD and Contracted PelvisДокумент55 страницCPD and Contracted PelvisShaells JoshiОценок пока нет
- Hip Disorders in Children DDHДокумент56 страницHip Disorders in Children DDHJulia WindiОценок пока нет
- Prenatal DiagnosisДокумент48 страницPrenatal DiagnosisReshop NandaОценок пока нет
- WCPD 2016 CP Diagnosis Treatment Infographic WORLDДокумент1 страницаWCPD 2016 CP Diagnosis Treatment Infographic WORLDvinicius_vrrОценок пока нет
- Pediatric Lower Extremity Orthopedic ConcernsДокумент28 страницPediatric Lower Extremity Orthopedic ConcernsDitaAnggaraKusumaОценок пока нет
- Lower Extremity DisordersДокумент25 страницLower Extremity DisordersJameson87Оценок пока нет
- Prenatal Diagnosis Techniques and Guidelines ExplainedДокумент29 страницPrenatal Diagnosis Techniques and Guidelines ExplainedNina Difla MuflikhahОценок пока нет
- Liveability Index 2022Документ13 страницLiveability Index 2022Jigga mannОценок пока нет
- Pehealth11 q2 Mod2of2 H.O.P.E v2Документ26 страницPehealth11 q2 Mod2of2 H.O.P.E v2Avillz Mar LeeОценок пока нет
- 7 HO Clearance Consent FormДокумент2 страницы7 HO Clearance Consent FormzanehfncbusinessОценок пока нет
- FA SSV3013 - Sem 2 2021 - 22Документ4 страницыFA SSV3013 - Sem 2 2021 - 22SITI ZUBAIDAH BINTI HALIMОценок пока нет
- Sustainable City PDFДокумент361 страницаSustainable City PDFagusbudiyonoОценок пока нет
- Republic of The Philippines Cordillera Administrative Region Municipality of TanudanДокумент1 страницаRepublic of The Philippines Cordillera Administrative Region Municipality of Tanudanpablo gayodanОценок пока нет
- Power Quality SolutionДокумент40 страницPower Quality Solutionshankar ammantryОценок пока нет
- ZDHCPNP V3.0Документ13 страницZDHCPNP V3.0Wendo BijaksonoОценок пока нет
- Clerking Sheet 1Документ8 страницClerking Sheet 1Precious ChaiОценок пока нет
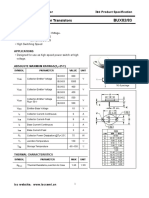
- Isc BUX82/83: Isc Silicon NPN Power TransistorsДокумент2 страницыIsc BUX82/83: Isc Silicon NPN Power TransistorsCarlos HCОценок пока нет
- Narcos 1x01 - DescensoДокумент53 страницыNarcos 1x01 - DescensoBirdy NumnumsОценок пока нет
- TuflineLinedBallValve 332148 2-07Документ12 страницTuflineLinedBallValve 332148 2-07Marcio NegraoОценок пока нет
- Autorefractometro GRK 7000Документ82 страницыAutorefractometro GRK 7000Wilson CepedaОценок пока нет
- Tinnitus Causes and TreatmentДокумент3 страницыTinnitus Causes and TreatmentTinnituscausesandtreatment Tinnituscausesandtreatment100% (1)
- Week 3. DIASДокумент14 страницWeek 3. DIASJaymie NeriОценок пока нет
- RRL - Airbag SystemДокумент3 страницыRRL - Airbag Systemclarice fОценок пока нет
- Disjointed.S01E03.720p.webrip.x264 STRiFE (Ettv) .SRTДокумент32 страницыDisjointed.S01E03.720p.webrip.x264 STRiFE (Ettv) .SRTArthur CarvalhoОценок пока нет
- Methyldopa Drug DataДокумент3 страницыMethyldopa Drug DataLaurel Joshua Reyes DauzОценок пока нет
- Cell Membrane TransportДокумент37 страницCell Membrane TransportMaya AwadОценок пока нет
- Homemade Litmus Paper ExperimentДокумент3 страницыHomemade Litmus Paper ExperimentEmmanuelle NazarenoОценок пока нет
- 7 Mineral and Soil ResourcesДокумент21 страница7 Mineral and Soil ResourcesShardy Lyn RuizОценок пока нет
- Timeline - Big BazaarДокумент4 страницыTimeline - Big BazaarKeerthana Lakshmi0% (1)
- Regulatory Updates on Japan's MO169 Medical Device Quality Management OrdinanceДокумент7 страницRegulatory Updates on Japan's MO169 Medical Device Quality Management OrdinanceHong XuyenОценок пока нет
- Eastern RlyДокумент25 страницEastern Rlyshivam.jhawar95Оценок пока нет
- Charles LawДокумент12 страницCharles LawLerr Real RelleОценок пока нет
- FP02BДокумент3 страницыFP02BRazak JeyОценок пока нет
- Play and Communication TheoryДокумент21 страницаPlay and Communication Theoryroberto100% (2)
- Sri Lanka's Economic Crisis Explained: Depleting Reserves, Food InflationДокумент11 страницSri Lanka's Economic Crisis Explained: Depleting Reserves, Food InflationRohan PachunkarОценок пока нет
- LPT22Документ3 страницыLPT22Leonardo Vinicio Olarte CarrilloОценок пока нет
- (Vikhroli West) : Raj LegacyДокумент4 страницы(Vikhroli West) : Raj LegacyNEHA NОценок пока нет