Вам также может понравиться
- Anti Parasites Blok 3.2Документ46 страницAnti Parasites Blok 3.2Alda Herlen Kalkarina BangunОценок пока нет
- AzithromycinДокумент4 страницыAzithromycinBrittany ClontzОценок пока нет
- Chemotherapy of Helminth Infections: DR - Rathnakar U.PДокумент39 страницChemotherapy of Helminth Infections: DR - Rathnakar U.PDr.U.P.Rathnakar.MD.DIH.PGDHMОценок пока нет
- ANTELMINTIKДокумент44 страницыANTELMINTIKnovi_linggaОценок пока нет
- Common Antibiotics Master List: Rodney Paullus Dewight Cowley Izzy Winestone Ben BowmanДокумент20 страницCommon Antibiotics Master List: Rodney Paullus Dewight Cowley Izzy Winestone Ben BowmanMahendra VermaОценок пока нет
- Therapy of Worm InfestationДокумент38 страницTherapy of Worm InfestationBishal ChauhanОценок пока нет
- Anti-Helminthic Drugs 27 11 2022Документ25 страницAnti-Helminthic Drugs 27 11 2022Exam IUBОценок пока нет
- Drug StudyДокумент8 страницDrug Studymaryhiromi10Оценок пока нет
- Farmakologi AntiparasitДокумент119 страницFarmakologi AntiparasitFitri Sri WulandariОценок пока нет
- Drugs Used To Treat: TuberculosisДокумент46 страницDrugs Used To Treat: TuberculosisDR AbidОценок пока нет
- Anthelmintics AgentsДокумент3 страницыAnthelmintics AgentsSimran SidhuОценок пока нет
- mebendazole-WPS OfficeДокумент6 страницmebendazole-WPS OfficeDenvicОценок пока нет
- ANTIMALARIAL DrugsДокумент25 страницANTIMALARIAL DrugsMANAS ChhapoliyaОценок пока нет
- ANTELMITIKДокумент51 страницаANTELMITIKAsti NurjanahОценок пока нет
- Oral Antifungal AgentsДокумент45 страницOral Antifungal AgentsIndah Febrini Triana JalalОценок пока нет
- Antibiotik Imipenem Golongan CarbapenemДокумент5 страницAntibiotik Imipenem Golongan Carbapenemabam_abamОценок пока нет
- Farmakologi Obat Kusta Dan Antiparasit 2015Документ84 страницыFarmakologi Obat Kusta Dan Antiparasit 2015Alex FerdinandОценок пока нет
- Farmakologi Obat Kusta Dan Antiparasit 2015Документ84 страницыFarmakologi Obat Kusta Dan Antiparasit 2015Alex FerdinandОценок пока нет
- Drug CardsДокумент187 страницDrug Cardsintaaf82% (33)
- Cefazolin AncefДокумент4 страницыCefazolin AncefAmanda La SalaОценок пока нет
- Protein Synth Inhibt and FluoroquinolonsДокумент28 страницProtein Synth Inhibt and FluoroquinolonsH.M. PiashОценок пока нет
- Urinary Germicides PharmaДокумент11 страницUrinary Germicides PharmaMaria Pina Barbado PonceОценок пока нет
- Antimalarial DrugsДокумент56 страницAntimalarial DrugsKasturiRangan SrivatsaОценок пока нет
- Topic 2.1: Antibiotics: Unit 2: Anti-Infective MedicationsДокумент50 страницTopic 2.1: Antibiotics: Unit 2: Anti-Infective MedicationsNirali ParmarОценок пока нет
- Pharmacology Anti Tubercular Drugs First LineДокумент26 страницPharmacology Anti Tubercular Drugs First LineFawad KhanОценок пока нет
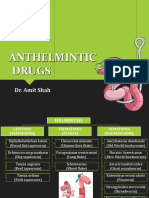
- Anthelmintic DrugsДокумент28 страницAnthelmintic DrugsAmit ShahОценок пока нет
- Anti Malarial DrugsДокумент42 страницыAnti Malarial DrugsSaurabh GautamОценок пока нет
- Antiparasitic Medications: Dr. Meera Ababneh, Pharm.D, PHDДокумент39 страницAntiparasitic Medications: Dr. Meera Ababneh, Pharm.D, PHDSaddamix AL OmariОценок пока нет
- Drugs Acting On The GitДокумент29 страницDrugs Acting On The GitIsheanesu MugwisiОценок пока нет
- Cancer Cell-Specific AgentsДокумент5 страницCancer Cell-Specific AgentsRomwella May AlgoОценок пока нет
- Antihelminths: DR Japhet Mangoyi Department of Clinical PharmacologyДокумент15 страницAntihelminths: DR Japhet Mangoyi Department of Clinical PharmacologyMitchelle SaurambaОценок пока нет
- EPIGENTДокумент3 страницыEPIGENTmahgad100% (1)
- Pharmacology Obat Lepra Dan TBC Kutis: Dharma Permana, PHD, AptДокумент33 страницыPharmacology Obat Lepra Dan TBC Kutis: Dharma Permana, PHD, AptanggiОценок пока нет
- Antibiotics in Pediatrics (Vancomycin, Quinolones, Aminoglycosides, Tetracyclines, Chloramphenicol, Clindamycin, Macrolides)Документ90 страницAntibiotics in Pediatrics (Vancomycin, Quinolones, Aminoglycosides, Tetracyclines, Chloramphenicol, Clindamycin, Macrolides)Jill PОценок пока нет
- CefaclorДокумент3 страницыCefaclorAyah PaasaОценок пока нет
- AmoxicillinДокумент2 страницыAmoxicillinjedisay1Оценок пока нет
- Antibiotik Dan Antiseptik Saluran KemihДокумент29 страницAntibiotik Dan Antiseptik Saluran KemihPutri Sari SeptirianiОценок пока нет
- Ciprofloxacin: A Drug Study OnДокумент5 страницCiprofloxacin: A Drug Study Onkarl montanoОценок пока нет
- Antibiotics in PeadiatricsДокумент14 страницAntibiotics in PeadiatricsrisanaОценок пока нет
- Anti - TB DrugsupdatedДокумент35 страницAnti - TB DrugsupdatedgОценок пока нет
- Dr. Anati Purwakanthi, MSC Departemen Farmakologi Fkik UnjaДокумент40 страницDr. Anati Purwakanthi, MSC Departemen Farmakologi Fkik Unjaanes tiraОценок пока нет
- Gentamycin: Classification of Antihypertensive DrugsДокумент3 страницыGentamycin: Classification of Antihypertensive DrugsMargo Milad Fahim SaadОценок пока нет
- Cytotoxic Drugs: Pharm. Dr. Ezekiel EfeobhokhanДокумент24 страницыCytotoxic Drugs: Pharm. Dr. Ezekiel EfeobhokhanjonaОценок пока нет
- 9 - Antiprotozoal DrugsДокумент29 страниц9 - Antiprotozoal Drugsمهند الرحيليОценок пока нет
- LevofloxacinДокумент2 страницыLevofloxacinEliza Rahardja100% (1)
- Name: Sophia Angela Famor BSN12EДокумент4 страницыName: Sophia Angela Famor BSN12EZumi IskakОценок пока нет
- Antimalarials DrugsДокумент27 страницAntimalarials DrugsAlishba MushtaqОценок пока нет
- Drug StudyДокумент7 страницDrug StudysarahtotОценок пока нет
- Treatment of Tuberculosis .2Документ59 страницTreatment of Tuberculosis .2Alexander Santiago Parel0% (1)
- Pharma-URO-CYCLIC LIPOEPETIDES (Vancomycin)Документ6 страницPharma-URO-CYCLIC LIPOEPETIDES (Vancomycin)Hussein AlhaddadОценок пока нет
- 12 MalariaДокумент61 страница12 MalariaMewael TesfamichaelОценок пока нет
- Cephalosporins, Flouroquinolones and SulfonamidesДокумент7 страницCephalosporins, Flouroquinolones and SulfonamidesErum JanОценок пока нет
- Pharma URO AminoglycosidesДокумент8 страницPharma URO AminoglycosidesHussein AlhaddadОценок пока нет
- AmoxitidДокумент5 страницAmoxitidelcapitano vegetaОценок пока нет
- IpsaДокумент19 страницIpsaLuisa LopezОценок пока нет
- Drug Monograph: Generic Name: Trade Name: Drug Class: IndicationsДокумент8 страницDrug Monograph: Generic Name: Trade Name: Drug Class: IndicationsRawan AlmutairiОценок пока нет
- AntibioticsДокумент58 страницAntibioticsKamal GhimireОценок пока нет
- Adult Infectious Disease Bulletpoints HandbookОт EverandAdult Infectious Disease Bulletpoints HandbookРейтинг: 4.5 из 5 звезд4.5/5 (9)
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryОт EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryОценок пока нет
- A Concise Overview On Heterocyclic Compounds Exhibiting Pesticidal ActivitiesДокумент16 страницA Concise Overview On Heterocyclic Compounds Exhibiting Pesticidal ActivitiesIJAR JOURNALОценок пока нет
- Free Closed Door Coaching Prof Arconado - Microbiology - 200 Items Key PDFДокумент14 страницFree Closed Door Coaching Prof Arconado - Microbiology - 200 Items Key PDFAnne MorenoОценок пока нет
- 2017 European Guidelines For The Management of Genital HerpesДокумент22 страницы2017 European Guidelines For The Management of Genital HerpesYanna RizkiaОценок пока нет
- 15 Healing Turmeric RecipesДокумент26 страниц15 Healing Turmeric Recipesemanvitoria100% (3)
- Western Mindanao State University College of Nursing Zamboanga CityДокумент16 страницWestern Mindanao State University College of Nursing Zamboanga CityRoshin TejeroОценок пока нет
- FLCCC Ivermectin in The Prophylaxis and Treatment of COVID 19Документ28 страницFLCCC Ivermectin in The Prophylaxis and Treatment of COVID 19brunorepettoОценок пока нет
- NCM 106 AntiviralДокумент34 страницыNCM 106 AntiviralJod BellОценок пока нет
- Dickinson 2020 Antiviral Treatment Using The Adeno PDFДокумент7 страницDickinson 2020 Antiviral Treatment Using The Adeno PDFNada HrenОценок пока нет
- Davis ProjectДокумент76 страницDavis ProjectMuhammad SameerОценок пока нет
- Writing-Data-Commentary SVC PART 2Документ81 страницаWriting-Data-Commentary SVC PART 2Mary Grace DimatacotОценок пока нет
- Antiviral TherapyДокумент4 страницыAntiviral Therapyanand dubeyОценок пока нет
- DDR PrimeДокумент4 страницыDDR PrimeNona AlyОценок пока нет
- Antiviral DrugsДокумент57 страницAntiviral DrugsInes Atas TupasОценок пока нет
- Momordica Charantia Linn. (Karela) : Nature's Silent HealerДокумент7 страницMomordica Charantia Linn. (Karela) : Nature's Silent Healerdaud faisalОценок пока нет
- 1918 Flu - How It HappenedДокумент7 страниц1918 Flu - How It Happenedhhelp12255Оценок пока нет
- Antivirals - DR Arundhati AbhyankarДокумент34 страницыAntivirals - DR Arundhati AbhyankarSiddhant BanwatОценок пока нет
- United States Patent Application - 0060257852 PDFДокумент297 страницUnited States Patent Application - 0060257852 PDFMatt OusleyОценок пока нет
- Development of Tamiflu and Relenza Fri 11th OctoberДокумент17 страницDevelopment of Tamiflu and Relenza Fri 11th Octoberap579Оценок пока нет
- Anti Viral Drugs: Maria Ulfah, M.Si., AptДокумент55 страницAnti Viral Drugs: Maria Ulfah, M.Si., AptFauzan NurohmanОценок пока нет
- GTS354 Semester Test 2 PrepДокумент15 страницGTS354 Semester Test 2 Prepreyneke.monyaОценок пока нет
- Application of Essential Oils As Natural Cosmetic PreservativesДокумент15 страницApplication of Essential Oils As Natural Cosmetic PreservativesjosareforОценок пока нет
- Colloidal Silver and Viral InfectionsДокумент13 страницColloidal Silver and Viral Infectionsspencerjonesy100% (7)
- Hes 005 - Pharmacology-P1 Exam: Total PointsДокумент18 страницHes 005 - Pharmacology-P1 Exam: Total PointsMaria OgabangОценок пока нет
- Medicament OsДокумент109 страницMedicament OsKatia ColonioОценок пока нет
- Antimicrobial AgentДокумент30 страницAntimicrobial AgentShardendu MishraОценок пока нет
- Unit 5 DiscussionДокумент7 страницUnit 5 DiscussionHugsОценок пока нет
- Chapter 67Документ1 страницаChapter 67James Gabriel SalardaОценок пока нет
- Bioactive Natural Compounds Against Human Coronavirus - 2020 - Acta PharmaceuticДокумент12 страницBioactive Natural Compounds Against Human Coronavirus - 2020 - Acta PharmaceuticMohammed Shuaib AhmedОценок пока нет
- Marine DrugsДокумент24 страницыMarine Drugsashwingggg100% (1)
- Acyclovir The Best Antiviral Drug Synthesis PaperДокумент7 страницAcyclovir The Best Antiviral Drug Synthesis Paperapi-309281593Оценок пока нет