Вам также может понравиться
- A System of Operative Surgery, Volume IV (of 4)От EverandA System of Operative Surgery, Volume IV (of 4)Рейтинг: 4 из 5 звезд4/5 (1)
- Billiary SystemДокумент60 страницBilliary SystemDONALD UNASHEОценок пока нет
- Bowel AnastomosisДокумент30 страницBowel AnastomosismrashaiedehОценок пока нет
- Pancreatic Cancer, Cystic Neoplasms and Endocrine Tumors: Diagnosis and ManagementОт EverandPancreatic Cancer, Cystic Neoplasms and Endocrine Tumors: Diagnosis and ManagementОценок пока нет
- Carcinomagallbladder PDFДокумент61 страницаCarcinomagallbladder PDFZaki DhiifОценок пока нет
- VaricoceleДокумент19 страницVaricoceleMariam AntonyОценок пока нет
- Extrahepatic Biliary ObstructionДокумент44 страницыExtrahepatic Biliary ObstructionOssama Abd Al-amierОценок пока нет
- Basics of Abdominal UltrasonographyДокумент141 страницаBasics of Abdominal UltrasonographyalmoslihОценок пока нет
- Congenital Anomalies of Urinary BladderДокумент102 страницыCongenital Anomalies of Urinary Bladdernancy voraОценок пока нет
- Baltarowich ABD pt1 Hepatobiliary US PDFДокумент22 страницыBaltarowich ABD pt1 Hepatobiliary US PDFEka KusumaningatiОценок пока нет
- Imaging of AdrenalsДокумент140 страницImaging of AdrenalsSahana RОценок пока нет
- Pancreatic Cancer: Aziz Ahmad, MD Surgical Oncology Mills-Peninsula Hospital April 23, 2011Документ18 страницPancreatic Cancer: Aziz Ahmad, MD Surgical Oncology Mills-Peninsula Hospital April 23, 2011mywifenoor1983Оценок пока нет
- Penetrating Abdominal TraumaДокумент3 страницыPenetrating Abdominal TraumaamrulОценок пока нет
- A Textbook On Surgical Short Cases 4nbsped 8190568132 9788190568135 CompressДокумент299 страницA Textbook On Surgical Short Cases 4nbsped 8190568132 9788190568135 CompressHamza Khan100% (1)
- 04 Esophageal TumorsДокумент36 страниц04 Esophageal TumorsDetty NoviantyОценок пока нет
- CA OesophagusДокумент47 страницCA OesophagusAnsif KОценок пока нет
- Faculty of Medicine NR - Ii Department of Surgery NR - Ii: Diseases of The Biliary TractДокумент40 страницFaculty of Medicine NR - Ii Department of Surgery NR - Ii: Diseases of The Biliary TractGalina LozovanuОценок пока нет
- Approach To Patients With Inguinoscrotal Masses: Section of Urology Department of Surgery The Medical CityДокумент43 страницыApproach To Patients With Inguinoscrotal Masses: Section of Urology Department of Surgery The Medical CityKevin Eric SantosОценок пока нет
- Benign Gynecological LesionsДокумент9 страницBenign Gynecological LesionsLanceОценок пока нет
- Ultrasound of Srotal Emergency in PediatricДокумент53 страницыUltrasound of Srotal Emergency in PediatricIsti Iryan PriantiОценок пока нет
- Gall Stone Disease: DR M.farhad General SurgeonДокумент56 страницGall Stone Disease: DR M.farhad General SurgeondrelvОценок пока нет
- Testicular TorsionДокумент12 страницTesticular TorsionlicutОценок пока нет
- Management of Anastomotic Complications of Colorectal SurgeryДокумент13 страницManagement of Anastomotic Complications of Colorectal Surgerydadupipa100% (1)
- Spleen Ultrasound: Dlshsi-Cmrt-000-Basics of Mri-NjegatchalianДокумент16 страницSpleen Ultrasound: Dlshsi-Cmrt-000-Basics of Mri-NjegatchalianJohn Andre RamosОценок пока нет
- Benign Disease of The Genital Tract by Hossam El SokkaryДокумент92 страницыBenign Disease of The Genital Tract by Hossam El Sokkarysalah subbahОценок пока нет
- Examination of The BreastДокумент10 страницExamination of The BreastHina MalikОценок пока нет
- 54.the Gallbladder and Bile DuctsДокумент19 страниц54.the Gallbladder and Bile DuctsAdenegan Adesola RaymondОценок пока нет
- Differential Diagnosis Pain Right HypochondriumДокумент35 страницDifferential Diagnosis Pain Right HypochondriumDrArish Mahmood100% (1)
- Bladder Outlet Obstruction in Children PDFДокумент64 страницыBladder Outlet Obstruction in Children PDFalaaОценок пока нет
- Directions: Each Question Below Contains Five Suggested Answers. Choose The One Best Response ToДокумент3 страницыDirections: Each Question Below Contains Five Suggested Answers. Choose The One Best Response ToTrottTamilОценок пока нет
- Benign and Malignant Lesion of Lower GIДокумент45 страницBenign and Malignant Lesion of Lower GIAhmad Alzu3beОценок пока нет
- D5 PolicyДокумент5 страницD5 PolicyDenis PogoreviciОценок пока нет
- Apr 28 Ultrasound Chawla PDFДокумент85 страницApr 28 Ultrasound Chawla PDFAna-Maria PopaОценок пока нет
- Kuliah Blok GI Tract - USG Abd - September 2010Документ65 страницKuliah Blok GI Tract - USG Abd - September 2010Natallia BatuwaelОценок пока нет
- LiverДокумент27 страницLiverAndi Arwan AgusnawanОценок пока нет
- 17 - Gallbladder StonesДокумент71 страница17 - Gallbladder StonesRashed Shatnawi100% (1)
- Pancreas and SpleenДокумент44 страницыPancreas and SpleenOgbuefi PascalОценок пока нет
- Rectal Cancer PPT 2.1Документ131 страницаRectal Cancer PPT 2.1Usmle GuyОценок пока нет
- Salivary Gland MalignanciesДокумент69 страницSalivary Gland MalignanciesKessi VikaneswariОценок пока нет
- Bosniak ClassificationДокумент19 страницBosniak ClassificationGirish Kumar100% (1)
- Colon, Rectum and AnusДокумент30 страницColon, Rectum and AnusKiara GovenderОценок пока нет
- Hernia: Inguinal - Surgical Anatomy, Presentation, Treatment, ComplicationsДокумент43 страницыHernia: Inguinal - Surgical Anatomy, Presentation, Treatment, ComplicationsFobin VargheseОценок пока нет
- Hepatocellular Carcinoma: Review ArticleДокумент13 страницHepatocellular Carcinoma: Review ArticleAnnagiulia Gramenzi100% (2)
- Case of Obstructive JaundiceДокумент38 страницCase of Obstructive JaundiceadiОценок пока нет
- Preparing Severely Jaundiced Patient For SurgeryДокумент2 страницыPreparing Severely Jaundiced Patient For Surgerylentini@maltanet.netОценок пока нет
- Thyroid GlandДокумент81 страницаThyroid Glanddr_shamimrОценок пока нет
- (Surg 3A) Spleen and Friends-Dr. Segismundo, Dr. Broqueza (Aisle Paler, Joseph Tolentino)Документ15 страниц(Surg 3A) Spleen and Friends-Dr. Segismundo, Dr. Broqueza (Aisle Paler, Joseph Tolentino)Aria Jean MostajoОценок пока нет
- Upper Gi BleedДокумент20 страницUpper Gi BleedNaeem Shehzad100% (1)
- Blunt Adominal TraumaДокумент14 страницBlunt Adominal TraumaMuhammad Bima AkbarОценок пока нет
- The Spleen - A Surgical Perspective: by Col. Abrar Hussain ZaidiДокумент43 страницыThe Spleen - A Surgical Perspective: by Col. Abrar Hussain Zaidiabrar_zaidiОценок пока нет
- Sentinel Lymph Node ConceptДокумент27 страницSentinel Lymph Node ConceptKarthikeyan RadhakrishnanОценок пока нет
- (SURG) 5.4b Management of Soft Tissue SarcomaДокумент6 страниц(SURG) 5.4b Management of Soft Tissue SarcomaKenneth TorresОценок пока нет
- Radiologi Kasus DigestifДокумент110 страницRadiologi Kasus DigestifarifgteguhОценок пока нет
- Scrotal SwellingДокумент40 страницScrotal Swellingeirene simbolonОценок пока нет
- Phyllodes TumorДокумент20 страницPhyllodes TumorManuela KarinaaОценок пока нет
- 12 Surgery For Critically Ill PatientsДокумент18 страниц12 Surgery For Critically Ill PatientsMyrtle Yvonne RagubОценок пока нет
- Coursebook-Livertransplant ch27Документ53 страницыCoursebook-Livertransplant ch27Сергей СадовниковОценок пока нет
- Kidney Part 1Документ5 страницKidney Part 1sarguss14Оценок пока нет
- Abdominal US in Hepatobiliary DiseasesДокумент76 страницAbdominal US in Hepatobiliary DiseasesSyafari D. MangopoОценок пока нет
- Benefits of HijamaДокумент3 страницыBenefits of HijamaBateria MeaОценок пока нет
- Maria's First Love and Tooth No. 29Документ2 страницыMaria's First Love and Tooth No. 29Doreene Andres0% (1)
- INTRODUCTIONДокумент3 страницыINTRODUCTIONSoumya Suguna TripathyОценок пока нет
- Carme Joy PRCДокумент6 страницCarme Joy PRCCarme Joy Panganiban LopezОценок пока нет
- Manualul Merck Editia 18 Limba Romana 161012115439 PDFДокумент36 страницManualul Merck Editia 18 Limba Romana 161012115439 PDFCristea MadalinaОценок пока нет
- Nodular Goiter Concept MapДокумент5 страницNodular Goiter Concept MapAllene PaderangaОценок пока нет
- OsteoporosisДокумент15 страницOsteoporosisWil LesterОценок пока нет
- Drug StudyДокумент4 страницыDrug StudyAilah Mae Dela Cruz0% (1)
- High Performance Eye Hospital: Shalini Nehra (80) - Sachin Nandanwar (75) - Subhash WagleДокумент45 страницHigh Performance Eye Hospital: Shalini Nehra (80) - Sachin Nandanwar (75) - Subhash WagleSachin Nandanwar100% (1)
- Regular Batch: Date DAY Theme TimeДокумент5 страницRegular Batch: Date DAY Theme TimeShweta DixitОценок пока нет
- Reckettsia and ChlamediaДокумент37 страницReckettsia and ChlamediaMuqtadir “The Ruler” KuchikiОценок пока нет
- Interventions of Postpartum Hemorrhage.16Документ17 страницInterventions of Postpartum Hemorrhage.16Fernando Peralta PalmezanoОценок пока нет
- Full List of Consortium Names and Affiliations Are Listed in The AppendixДокумент60 страницFull List of Consortium Names and Affiliations Are Listed in The AppendixJohnОценок пока нет
- Instilling Otic/Ear Drops Procedure RationaleДокумент12 страницInstilling Otic/Ear Drops Procedure RationaleBSN2-F MASINING NA PAGPAPAHAYAGОценок пока нет
- Maybury ManualДокумент55 страницMaybury ManualFriends of MayburyОценок пока нет
- Blood Collection TubesДокумент1 страницаBlood Collection TubesMohammad Atiq100% (1)
- PRO III 2012 Long Case (Surgical)Документ39 страницPRO III 2012 Long Case (Surgical)vijayaОценок пока нет
- Causes of InflammationДокумент1 страницаCauses of InflammationZainab KhanОценок пока нет
- Third Quarter Science 10 - BiologyДокумент91 страницаThird Quarter Science 10 - BiologyApple ArellanoОценок пока нет
- PMLS LecДокумент4 страницыPMLS LecAlyana GabiniОценок пока нет
- VermiphobiaДокумент2 страницыVermiphobiaKenPedresoОценок пока нет
- 1487910656-1. Dr. Reno-1Документ20 страниц1487910656-1. Dr. Reno-1IvanRaykaОценок пока нет
- Hypertension NCLEX Quiz Questions: A. I Will Make Sure I Consume Foods High in PotassiumДокумент5 страницHypertension NCLEX Quiz Questions: A. I Will Make Sure I Consume Foods High in PotassiumMelodia Turqueza GandezaОценок пока нет
- Visual Acuity: Opthalmology CEX StepsДокумент5 страницVisual Acuity: Opthalmology CEX StepsVanessa HermioneОценок пока нет
- The Human Eye PowerPointДокумент69 страницThe Human Eye PowerPointKemoy Francis100% (1)
- LET Contacts 10-14Документ4 страницыLET Contacts 10-14Wayne MaughanОценок пока нет
- Non Kepi Vaccines RevisedДокумент28 страницNon Kepi Vaccines Revisedokwadha simionОценок пока нет
- Twin Block Case ReportДокумент5 страницTwin Block Case ReportwjeelaniОценок пока нет
- Active Cycle of Breathing TechniqueДокумент2 страницыActive Cycle of Breathing TechniqueKurniawaty SupriyadiОценок пока нет
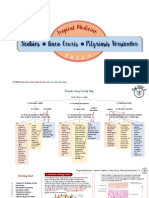
- Scabies Tinea Cruris Pityriasis Versicolor: Semangat!Документ11 страницScabies Tinea Cruris Pityriasis Versicolor: Semangat!Fitriah Nur SyamiatiОценок пока нет