Вам также может понравиться
- Trochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandTrochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Excessive Genu Valgum FINALДокумент13 страницExcessive Genu Valgum FINALMeeraОценок пока нет
- Forearm Fractures, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandForearm Fractures, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Club FootДокумент5 страницClub FootanisadestyaОценок пока нет
- Hip Neck Fracture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHip Neck Fracture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Genu Valgus Genu VarusДокумент35 страницGenu Valgus Genu VarusRatu FaniaОценок пока нет
- Hip Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentОт EverandHip Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentОценок пока нет
- Hip Examination in The ChildДокумент24 страницыHip Examination in The ChildDharmendra WidetyaОценок пока нет
- Hallux Varus, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHallux Varus, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- PHTH 492 - Orthotics & Prosthetics Syllabus-2023Документ14 страницPHTH 492 - Orthotics & Prosthetics Syllabus-2023HATUN AYED ALOBAIDIОценок пока нет
- Bow Leg (Final) 3.9.20Документ23 страницыBow Leg (Final) 3.9.20Gerald EthelieОценок пока нет
- Genu Recurvatum SyndromДокумент7 страницGenu Recurvatum SyndromRoxana RascaОценок пока нет
- Genovarum and GenovalgumДокумент7 страницGenovarum and GenovalgumVerli Fajriati NofliОценок пока нет
- OSTEOTOMIES AROUND THE HIP FinalДокумент51 страницаOSTEOTOMIES AROUND THE HIP FinalWasim R. IssaОценок пока нет
- AO Trauma Vol.2Документ100 страницAO Trauma Vol.2Cujba GheorgheОценок пока нет
- Distal Femur (Sandeep Sir)Документ22 страницыDistal Femur (Sandeep Sir)Kirubakaran Saraswathy PattabiramanОценок пока нет
- Hip OsteotmyДокумент4 страницыHip OsteotmyAhmed KeshkОценок пока нет
- Osteotomias PediatriaДокумент13 страницOsteotomias PediatriaM Ram CrraОценок пока нет
- B 756 Vertebris GB III10Документ44 страницыB 756 Vertebris GB III10Lukasz Bartochowski100% (1)
- Shoulder Dislocation DraftДокумент26 страницShoulder Dislocation Drafthusnajihah18Оценок пока нет
- Musculoskeletal TraumaДокумент103 страницыMusculoskeletal TraumaJona Kristin EnclunaОценок пока нет
- Management of The Floating Knee.Документ8 страницManagement of The Floating Knee.barbara liuva chia policarpoОценок пока нет
- Pes Planus - Synopsis of CausationДокумент14 страницPes Planus - Synopsis of CausationSari HestiyariniОценок пока нет
- Sem Osteoporosis (Edit)Документ31 страницаSem Osteoporosis (Edit)Rhomizal MazaliОценок пока нет
- Erbs PalsyДокумент9 страницErbs PalsyVatsalVermaОценок пока нет
- Acute Management Pelvic RingДокумент91 страницаAcute Management Pelvic RingClever ImaniaОценок пока нет
- Club Foot-Dr J SahooДокумент9 страницClub Foot-Dr J SahooSheel Gupta100% (1)
- AAOS2007 Pediatric PDFДокумент58 страницAAOS2007 Pediatric PDFHéctor Pando SánchezОценок пока нет
- Perthes Disease: Mohamed Hamood MohamedДокумент4 страницыPerthes Disease: Mohamed Hamood MohamedMohamed HamoodОценок пока нет
- Achilles Tendon RuptureДокумент19 страницAchilles Tendon Ruptureapi-509245925Оценок пока нет
- Lower Extremity DisordersДокумент25 страницLower Extremity DisordersJameson87Оценок пока нет
- External Fixation Principles and Applications.5Документ8 страницExternal Fixation Principles and Applications.5Leonardo Rocha100% (1)
- C SpineДокумент33 страницыC SpineKarthickОценок пока нет
- Hip Joint 1Документ22 страницыHip Joint 1foziiiii100% (2)
- Shoulder Dislocation TechniquesДокумент9 страницShoulder Dislocation TechniqueskenthepaОценок пока нет
- Lower Limb Deformity in ChildrenДокумент13 страницLower Limb Deformity in ChildrenShyra RahmnОценок пока нет
- Flexor Tendon Injuries SeminarДокумент75 страницFlexor Tendon Injuries SeminarAmit GoyalОценок пока нет
- Developmental Hip Dysplasia and DislocationДокумент51 страницаDevelopmental Hip Dysplasia and Dislocationandi firdha restuwatiОценок пока нет
- Toe and Foot ConditionsДокумент14 страницToe and Foot ConditionsNur InsyirahОценок пока нет
- Anterior Cruciate Ligament Surgery: Trauma & Orthopaedic DirectorateДокумент38 страницAnterior Cruciate Ligament Surgery: Trauma & Orthopaedic DirectorateSzilvia MartonosОценок пока нет
- Spinal Trauma: Causes of Cervical Spinal Injury (UK)Документ16 страницSpinal Trauma: Causes of Cervical Spinal Injury (UK)Mohamed Farouk El-FaresyОценок пока нет
- Proximal Femoral NewДокумент34 страницыProximal Femoral NewHimanshu HemantОценок пока нет
- ACL Injury PresentationДокумент36 страницACL Injury Presentationmail_rajibОценок пока нет
- Precautions Following Hemiarthoplasty PDFДокумент8 страницPrecautions Following Hemiarthoplasty PDFdrprashantmb1012Оценок пока нет
- Tennis ElbowДокумент13 страницTennis ElbowPadma PadalОценок пока нет
- Management of FractureДокумент20 страницManagement of FractureHitesh RohitОценок пока нет
- Pediatrics FracturesДокумент14 страницPediatrics Fracturesخالد الغامديОценок пока нет
- Achilles RuptureДокумент23 страницыAchilles RupturePhysiotherapist AliОценок пока нет
- Lower Limb Fracture..MeДокумент142 страницыLower Limb Fracture..MeWorku KifleОценок пока нет
- Oh My Painful FOOT!!!: Plantar FasciitisДокумент20 страницOh My Painful FOOT!!!: Plantar FasciitisAsogaa MeteranОценок пока нет
- Gpe - 017.1 - Orthopaedic ExaminationДокумент3 страницыGpe - 017.1 - Orthopaedic ExaminationImiey Eleena HanumОценок пока нет
- Jurnal Shoulder Dislocation - PendekДокумент84 страницыJurnal Shoulder Dislocation - PendekCliff LewisОценок пока нет
- Hemiarthroplasty Hip - Apr20Документ10 страницHemiarthroplasty Hip - Apr20Shalu OjhaОценок пока нет
- Distal Femur Fractures Fixation by Locking Compression Plate-Assessment of Outcome by Rasmussens Functional Knee ScoreДокумент7 страницDistal Femur Fractures Fixation by Locking Compression Plate-Assessment of Outcome by Rasmussens Functional Knee ScoreIJAR JOURNALОценок пока нет
- Acl Injury Surgery - Orthoinfo - AaosДокумент15 страницAcl Injury Surgery - Orthoinfo - Aaosapi-228773845Оценок пока нет
- Ctev NewДокумент48 страницCtev NewDhinie NovianiОценок пока нет
- DRUJinstabilityreview - PDF 034407Документ15 страницDRUJinstabilityreview - PDF 034407Oscar Cayetano Herrera RodríguezОценок пока нет
- Long Case OrthopaedicДокумент24 страницыLong Case OrthopaedicSyimah UmarОценок пока нет
- Examination of The Knee Joint - RP's Ortho NotesДокумент3 страницыExamination of The Knee Joint - RP's Ortho NotesSabari NathОценок пока нет
- Review - Presby Residency ManualДокумент400 страницReview - Presby Residency ManualSneha SutharОценок пока нет
- The Case of The Reference On The Pathology Delivery and ParturitionДокумент4 страницыThe Case of The Reference On The Pathology Delivery and ParturitionPutri DwiridalОценок пока нет
- PRENATAL CARE PuputДокумент8 страницPRENATAL CARE PuputPutri DwiridalОценок пока нет
- PielobefritisДокумент9 страницPielobefritisPutri DwiridalОценок пока нет
- Congenital Abnormalities On Women Oleh PuputДокумент26 страницCongenital Abnormalities On Women Oleh PuputPutri DwiridalОценок пока нет
- Congenital Abnormalities On Women Oleh PuputДокумент26 страницCongenital Abnormalities On Women Oleh PuputPutri DwiridalОценок пока нет
- Drug Resistance in TuberculosisДокумент4 страницыDrug Resistance in TuberculosisPutri DwiridalОценок пока нет
- Pleas Join Us For A Luncheon Celebrating: You Are InvitedДокумент3 страницыPleas Join Us For A Luncheon Celebrating: You Are InvitedPutri DwiridalОценок пока нет
- Narative Siap PrintДокумент1 страницаNarative Siap PrintPutri DwiridalОценок пока нет
- Prenatal Care, Prevention of Labor and Postpartum ComplicationsДокумент8 страницPrenatal Care, Prevention of Labor and Postpartum ComplicationsPutri DwiridalОценок пока нет
- ADJEKTIFДокумент5 страницADJEKTIFPutri DwiridalОценок пока нет
- LOVE From The Heart HHI MagazineДокумент35 страницLOVE From The Heart HHI MagazineCristina SarbuОценок пока нет
- Herpes Simplex Oral: EpidemiologyДокумент5 страницHerpes Simplex Oral: EpidemiologyFariz RamadhanОценок пока нет
- Hiv 101Документ33 страницыHiv 101Hend Al-RamahiОценок пока нет
- Wallen Et Al-2006-Australian Occupational Therapy JournalДокумент1 страницаWallen Et Al-2006-Australian Occupational Therapy Journal胡知行Оценок пока нет
- Mental Illness and HomelessnessДокумент2 страницыMental Illness and HomelessnessLauren FaustОценок пока нет
- Fin e 171 2014 PDFДокумент66 страницFin e 171 2014 PDFRenugopalОценок пока нет
- Maternal and Child Nursing QuestionsДокумент87 страницMaternal and Child Nursing QuestionsAnn Michelle Tarrobago50% (2)
- Biochemistry of Bitterness in Bamboo Shoots: Debangana Choudhury, Jatindra K. Sahu and G. D. SharmaДокумент7 страницBiochemistry of Bitterness in Bamboo Shoots: Debangana Choudhury, Jatindra K. Sahu and G. D. SharmaKuo SarongОценок пока нет
- Collaborative Couple Therapy: Page Pr/gurman3.htm&dir Pp/fac&cart - IdДокумент39 страницCollaborative Couple Therapy: Page Pr/gurman3.htm&dir Pp/fac&cart - IdCarlos InfanteОценок пока нет
- Meyer-Grieve James Et AlДокумент9 страницMeyer-Grieve James Et Aljolamo1122916Оценок пока нет
- Measles (Campak, Rubeola, Gabak, Kerumut)Документ20 страницMeasles (Campak, Rubeola, Gabak, Kerumut)Ami UtamiatiОценок пока нет
- Designer Babies For Reading Packet 1Документ4 страницыDesigner Babies For Reading Packet 1Amirah Hadi AqilahОценок пока нет
- What Is Alzheimer's - Alzheimer's AssociationДокумент6 страницWhat Is Alzheimer's - Alzheimer's AssociationRatnaPrasadNalamОценок пока нет
- Gestalt Sept2019 FINALДокумент3 страницыGestalt Sept2019 FINALMolly ChristensenОценок пока нет
- Bipolar DisordersДокумент63 страницыBipolar DisorderselvinegunawanОценок пока нет
- Emergency Department Handbook PDFДокумент461 страницаEmergency Department Handbook PDFdmallozziОценок пока нет
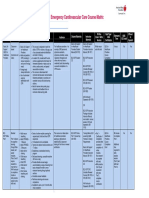
- Emergency Cardiovascular Care Course MatrixДокумент15 страницEmergency Cardiovascular Care Course MatrixJesus M. Espinosa EchavarriaОценок пока нет
- CHFДокумент35 страницCHFNurayunie Abd HalimОценок пока нет
- Scio and Its Functionality and UsesДокумент5 страницScio and Its Functionality and UsesAndy MilitaruОценок пока нет
- Ankylosing SpondylitisДокумент4 страницыAnkylosing SpondylitisHenry TirtosuhartoОценок пока нет
- Anestesi Obat ObatanДокумент72 страницыAnestesi Obat ObatanfujiОценок пока нет
- EcotherapyДокумент2 страницыEcotherapygeraldinmccaul85Оценок пока нет
- Crisis CounsellingДокумент28 страницCrisis CounsellingPooja varmaОценок пока нет
- Nursereview Org Therapeutic Communication TechniquesДокумент6 страницNursereview Org Therapeutic Communication TechniquesPatricia VasquezОценок пока нет
- Child Psychopathology: Child Psychopathology Is The Manifestation of Psychological Disorders in Children andДокумент7 страницChild Psychopathology: Child Psychopathology Is The Manifestation of Psychological Disorders in Children andMarvellous MunhuwaОценок пока нет
- Obstetric Analgesia PDFДокумент45 страницObstetric Analgesia PDFBoneyJalgar100% (1)
- Wart Removal and TreatmentДокумент6 страницWart Removal and TreatmentwandaОценок пока нет
- Myopia APDF PDFДокумент14 страницMyopia APDF PDFRao Sab100% (1)
- CBT For Panic DisorderДокумент40 страницCBT For Panic Disordersavvy_as_98100% (1)
- Pranashakty EbrochureДокумент6 страницPranashakty EbrochureMuay KhanОценок пока нет