Вам также может понравиться
- Basic of Thorax ImagingДокумент105 страницBasic of Thorax ImagingIlham Matoha100% (1)
- Imaging in Genitourinary SystemДокумент77 страницImaging in Genitourinary SystemIrvan R. Loho100% (1)
- Gambaran Radiologi AtelektasisДокумент40 страницGambaran Radiologi AtelektasisRaymond Frazier100% (1)
- Radiology SpottersДокумент24 страницыRadiology SpottersSameer VermaОценок пока нет
- Interpretasi Thorax FotoДокумент38 страницInterpretasi Thorax FotoElfha MonitaОценок пока нет
- Surgery I #3 - Fluid and ElectrolytesДокумент9 страницSurgery I #3 - Fluid and ElectrolytesCarl Earvin L. Favorito100% (1)
- Gambaran Radiologi ThoraxДокумент23 страницыGambaran Radiologi ThoraxAchmad MuhazirОценок пока нет
- Step 2 CK NBME 6 (Q)Документ184 страницыStep 2 CK NBME 6 (Q)M. Baidar SaeedОценок пока нет
- Radiology EssentialsДокумент308 страницRadiology EssentialsDeborah Anasthasia PakpahanОценок пока нет
- Polycythemia Vera: Kimberly Truong Wendy YangДокумент22 страницыPolycythemia Vera: Kimberly Truong Wendy YangAdeena RayОценок пока нет
- The Liver Imaging-Reporting and Data System (Li-RadsДокумент10 страницThe Liver Imaging-Reporting and Data System (Li-RadsserubimОценок пока нет
- Epilepsy in PregnancyДокумент20 страницEpilepsy in Pregnancytenri olaОценок пока нет
- Psychiatric Practice TestДокумент4 страницыPsychiatric Practice TestARIS100% (1)
- Soal Ujian RadiologiДокумент4 страницыSoal Ujian RadiologiTania Febrina100% (1)
- NuclearMedicineMedicalStudents LecturesДокумент197 страницNuclearMedicineMedicalStudents LecturesCosmin ConstantinОценок пока нет
- Drug Study On MAGNESIUM SULFATEДокумент6 страницDrug Study On MAGNESIUM SULFATEshadow gonzalezОценок пока нет
- Post Anesthesia RecoveryДокумент69 страницPost Anesthesia RecoverypaulaОценок пока нет
- NAN KE ANDROLOGY Yang Wei - Erectile Dysfunction From Chinese Medicine and BiomedicalДокумент100 страницNAN KE ANDROLOGY Yang Wei - Erectile Dysfunction From Chinese Medicine and BiomedicalLeo100% (1)
- BCS RadiologiДокумент46 страницBCS RadiologiHananya Manroe100% (1)
- Radiology Examination For Tractus Digestivus Chairunnisa, Dr. SP - RadДокумент100 страницRadiology Examination For Tractus Digestivus Chairunnisa, Dr. SP - RadDiana OCtavinaОценок пока нет
- Pneumology 2018Документ16 страницPneumology 2018Kris100% (1)
- Loopography Examination For Colon Cancer 7c394e77Документ11 страницLoopography Examination For Colon Cancer 7c394e77N. Camelya FirdausОценок пока нет
- Cardiac ImagingДокумент27 страницCardiac ImagingViorelVelenciucОценок пока нет
- CHD2 - DR Shirley L AДокумент74 страницыCHD2 - DR Shirley L ARaihan Luthfi100% (1)
- Anatomi RadiologiДокумент16 страницAnatomi RadiologiIncy CyvaОценок пока нет
- Teknik Pemeriksaan Vertebrae1Документ37 страницTeknik Pemeriksaan Vertebrae1Dadding DaddiОценок пока нет
- Unusual Presentation of Pancreatic Insulinoma:a Case ReportДокумент5 страницUnusual Presentation of Pancreatic Insulinoma:a Case ReportIJAR JOURNALОценок пока нет
- Latihan EkspertiseДокумент40 страницLatihan EkspertiseRoberto HutapeaОценок пока нет
- Review Jurnal RadiologiДокумент10 страницReview Jurnal RadiologiM Benni KadapihОценок пока нет
- Introduction To Clinical Radiology: The Breast: Priscilla J. Slanetz MD, MPH Assistant Professor of RadiologyДокумент10 страницIntroduction To Clinical Radiology: The Breast: Priscilla J. Slanetz MD, MPH Assistant Professor of Radiologydrqazi777Оценок пока нет
- BVCUGДокумент13 страницBVCUGyulianpatriawanОценок пока нет
- Midgut Volvulus 2018Документ2 страницыMidgut Volvulus 2018zzzОценок пока нет
- Dasar-Dasar Radiologi Musculoskeletal PDFДокумент101 страницаDasar-Dasar Radiologi Musculoskeletal PDFIndra MahaputraОценок пока нет
- Jurnal RadiologiДокумент8 страницJurnal RadiologiNia Nurhayati ZakiahОценок пока нет
- Kuliah Radiologi Emergensi - Maret 2020 - PlainДокумент67 страницKuliah Radiologi Emergensi - Maret 2020 - PlainArief VerditoОценок пока нет
- GI Tract: DR - Yanto Budiman. SP - Rad, M.Kes Bagian Radiologi FK/RS. Atma JayaДокумент94 страницыGI Tract: DR - Yanto Budiman. SP - Rad, M.Kes Bagian Radiologi FK/RS. Atma JayaNatallia BatuwaelОценок пока нет
- Pemeriksaan Radiologi Pada Sistem Respirasi01Документ115 страницPemeriksaan Radiologi Pada Sistem Respirasi01Rendy NunuhituОценок пока нет
- DR - Dr. Tahan P.H.,: FK UWK Surabaya Januari 2014Документ30 страницDR - Dr. Tahan P.H.,: FK UWK Surabaya Januari 2014Chen SiongОценок пока нет
- Pelvic Fractures - Experience of Pelvic Ring Fractures at A Major Trauma CentreДокумент8 страницPelvic Fractures - Experience of Pelvic Ring Fractures at A Major Trauma CentreFatrika DewiОценок пока нет
- Abdomen GIT Radiology 1Документ57 страницAbdomen GIT Radiology 1malekОценок пока нет
- Px. Abdomen RadiologiДокумент46 страницPx. Abdomen RadiologiwagigtnОценок пока нет
- FistulografiДокумент11 страницFistulografiAisa MaulidianaОценок пока нет
- DextrocardiaДокумент10 страницDextrocardiaJellie MendozaОценок пока нет
- Kuliah Untar Gi TractДокумент97 страницKuliah Untar Gi TractNisha YulitaОценок пока нет
- GossipybomaДокумент8 страницGossipybomaDADDYTOОценок пока нет
- Expertise Fam NikiДокумент5 страницExpertise Fam NikiNiki Rizqi rachmawatiОценок пока нет
- Radiographic Positioning and Related Anatomy by Isadore MeschanДокумент3 страницыRadiographic Positioning and Related Anatomy by Isadore MeschanChe Castro0% (1)
- Kuliah Radiologi - DR - DR.JB - Prasodjo, SpradДокумент47 страницKuliah Radiologi - DR - DR.JB - Prasodjo, SpradBrian MillerОценок пока нет
- Emergency Radiology PDFДокумент41 страницаEmergency Radiology PDFRobiul AlamОценок пока нет
- DAFTAR PUSTAKA RadiologiДокумент1 страницаDAFTAR PUSTAKA RadiologiSantrii AdztiiОценок пока нет
- E-Cube 9 Diamond CatalogДокумент14 страницE-Cube 9 Diamond CatalogJose QuiscaОценок пока нет
- 4.menajemen Dokter Penunjang Radiologi, Clinical Reasoning SM 7. 2011Документ35 страниц4.menajemen Dokter Penunjang Radiologi, Clinical Reasoning SM 7. 2011Pradipta SuarsyafОценок пока нет
- Pictorial Essay: Multidetector CT Urography With Abdominal Compression and Three-Dimensional ReconstructionДокумент13 страницPictorial Essay: Multidetector CT Urography With Abdominal Compression and Three-Dimensional ReconstructionHarley Alejo MОценок пока нет
- 1 OMD, Indikasi, Dan Mekanisme Rujukan PanoramicДокумент57 страниц1 OMD, Indikasi, Dan Mekanisme Rujukan PanoramicDian KafahasindayaОценок пока нет
- Congenital Tibia HemimeliaДокумент19 страницCongenital Tibia HemimeliaAlfred JacksonОценок пока нет
- Radiologi Kasus DigestifДокумент110 страницRadiologi Kasus DigestifarifgteguhОценок пока нет
- Ileus - Prof - Bachtiar Murtala (PP) PDFДокумент37 страницIleus - Prof - Bachtiar Murtala (PP) PDFAchmad Rizki AlhasaniОценок пока нет
- Sickle Cell DiseaseДокумент22 страницыSickle Cell DiseaseDias SetiawanОценок пока нет
- Volvulus Characterization in Radiology: A Review: Poster No.: Congress: Type: Topic: AuthorsДокумент21 страницаVolvulus Characterization in Radiology: A Review: Poster No.: Congress: Type: Topic: AuthorsAgunkRestuMaulanaОценок пока нет
- Gambaran Radiologi Arthritis SeptikДокумент6 страницGambaran Radiologi Arthritis SeptikIndira MaycellaОценок пока нет
- Worksheet PrognosisДокумент3 страницыWorksheet PrognosisAmieyAtlantaMayОценок пока нет
- TB and Lung CancerДокумент26 страницTB and Lung CanceraprinaaaОценок пока нет
- Abdominal ImagingДокумент45 страницAbdominal ImagingFahriansyah Mp Tmc100% (1)
- Foto Waters: Sinus Frontalis Dex-Sin N, Sinmax Sin TMPK Prselubungan, Sinmax Dex N, Sin Ethmoid Dex-Sin N, Sin Spenoidalis Dex-Sin N, tlg2 NДокумент25 страницFoto Waters: Sinus Frontalis Dex-Sin N, Sinmax Sin TMPK Prselubungan, Sinmax Dex N, Sin Ethmoid Dex-Sin N, Sin Spenoidalis Dex-Sin N, tlg2 NVita SariОценок пока нет
- Fetal Neural Tube 2021 12 LMBR PDFДокумент24 страницыFetal Neural Tube 2021 12 LMBR PDFwayansiagaОценок пока нет
- Slide Perbedaan Appendicitis Akut, Appendicitis Infiltrat Dan AbsesДокумент30 страницSlide Perbedaan Appendicitis Akut, Appendicitis Infiltrat Dan AbsesJessica Giovanni RuntuОценок пока нет
- Telaah Kritis JurnalДокумент13 страницTelaah Kritis JurnalfebrinaОценок пока нет
- Chest X. Rays InterpretationsДокумент39 страницChest X. Rays InterpretationsMohamad KarimaОценок пока нет
- Efektifitas Penggunaan Kasur Anti Dekubitus Dengan Terapi Pijatan Pada Pencegahan Dekubitus Terhadap Pasien Tirah Baring Rsud Undata PaluДокумент6 страницEfektifitas Penggunaan Kasur Anti Dekubitus Dengan Terapi Pijatan Pada Pencegahan Dekubitus Terhadap Pasien Tirah Baring Rsud Undata Palumafoel39Оценок пока нет
- Interpretasi Hasil Analisa Gas Darah: (Formula Anderson-Hasselbach)Документ28 страницInterpretasi Hasil Analisa Gas Darah: (Formula Anderson-Hasselbach)mafoel39Оценок пока нет
- CPG Management of Acute ST Segment Elevation Myocardial Infarction (2nd Edition)Документ64 страницыCPG Management of Acute ST Segment Elevation Myocardial Infarction (2nd Edition)Quah Yen YeeОценок пока нет
- Face Fracture Treatment & Management: Prehospital CareДокумент7 страницFace Fracture Treatment & Management: Prehospital Caremafoel39Оценок пока нет
- Face Fracture Treatment & Management: Prehospital CareДокумент7 страницFace Fracture Treatment & Management: Prehospital Caremafoel39Оценок пока нет
- Aplastic Anemia Pa Tho PhysiologyДокумент3 страницыAplastic Anemia Pa Tho Physiologyneil052275% (4)
- 93 - 08 Bantar 7 Hal 306-312Документ7 страниц93 - 08 Bantar 7 Hal 306-312amilyapraditaОценок пока нет
- Day 12 - Ncm-109 7b InfancyДокумент59 страницDay 12 - Ncm-109 7b InfancySheena Patricia ArasulaОценок пока нет
- DM, DKA, and IDMДокумент19 страницDM, DKA, and IDMJennyu YuОценок пока нет
- GeriatricsДокумент108 страницGeriatricsQasim AwanОценок пока нет
- Common Symptoms of Gastrointestinal and Abdominal DiseaseДокумент34 страницыCommon Symptoms of Gastrointestinal and Abdominal DiseaseMalueth AnguiОценок пока нет
- Start CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorДокумент2 страницыStart CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorFelicia ErikaОценок пока нет
- The Medical Management of Abnormal Uterine Bleeding in Reproductive-Aged WomenДокумент14 страницThe Medical Management of Abnormal Uterine Bleeding in Reproductive-Aged Womendiegoesteban1234Оценок пока нет
- Stugeron ForteДокумент4 страницыStugeron ForteJemsMei Comparativo MensuradoОценок пока нет
- Skin Rashes: An Emerging Symptom of COVID-19: What Clinicians Need To Know About Cutaneous Manifestations of COVID-19Документ3 страницыSkin Rashes: An Emerging Symptom of COVID-19: What Clinicians Need To Know About Cutaneous Manifestations of COVID-19littlemisseeeОценок пока нет
- Pharmanutrition: Yoichi Sunagawa, Yasufumi Katanasaka, Koji Hasegawa, Tatsuya MorimotoДокумент5 страницPharmanutrition: Yoichi Sunagawa, Yasufumi Katanasaka, Koji Hasegawa, Tatsuya MorimotoRizky AmaliaОценок пока нет
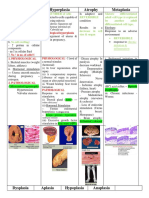
- Hypertrophy Hyperplasia Atrophy MetaplasiaДокумент20 страницHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanОценок пока нет
- Causes of Ischemic Stroke: October 2010Документ19 страницCauses of Ischemic Stroke: October 2010Pajokka 10Оценок пока нет
- Dipiros Pharmacotherapy Handbook 12Th Edition Terry L Schwinghammer Full ChapterДокумент67 страницDipiros Pharmacotherapy Handbook 12Th Edition Terry L Schwinghammer Full Chapterian.costa277100% (13)
- Fasciculation in Amyotrophic Lateral Sclerosis - Origin and Pathophysiological RelevanceДокумент8 страницFasciculation in Amyotrophic Lateral Sclerosis - Origin and Pathophysiological RelevanceConstanza SalgadoОценок пока нет
- High Anion Gap Metabolic AcidosisДокумент6 страницHigh Anion Gap Metabolic AcidosisharvardboyОценок пока нет
- 1 Anti Emetics II BDS 3 June 2020 AdobeДокумент28 страниц1 Anti Emetics II BDS 3 June 2020 AdobeBishal ChauhanОценок пока нет
- Epidemiology of Snake BitesДокумент19 страницEpidemiology of Snake BitesJonathan JumalonОценок пока нет
- ParalysisДокумент4 страницыParalysissakuraleeshaoranОценок пока нет
- Imp PhysiologyДокумент16 страницImp PhysiologysipransinghОценок пока нет
- Omalizumab - Drug Information - UpToDate-4Документ5 страницOmalizumab - Drug Information - UpToDate-4Vh TRОценок пока нет
- Muscle Weakness in Adults PDFДокумент14 страницMuscle Weakness in Adults PDFJames TianОценок пока нет