Вам также может понравиться
- Lower Resp TraumaДокумент62 страницыLower Resp TraumaA Rezki ChairamsyahОценок пока нет
- 6 PneumothoraxДокумент25 страниц6 PneumothoraxRana VandanaОценок пока нет
- Chest TraumaДокумент39 страницChest Traumayared getachewОценок пока нет
- Nursing Care of Patients With Pneumothorax: Prepared By: N. WadeДокумент33 страницыNursing Care of Patients With Pneumothorax: Prepared By: N. WadeokaciaОценок пока нет
- Chapter 16: Ready For ReviewДокумент5 страницChapter 16: Ready For Reviewsamfarmer333Оценок пока нет
- Lung SurgeriesДокумент43 страницыLung SurgeriesSereinОценок пока нет
- Traumatic Chest InjuryДокумент26 страницTraumatic Chest InjurySarahОценок пока нет
- Advanced Trauma Life Support (Atls) : DR Eko Setiawan, SpotДокумент67 страницAdvanced Trauma Life Support (Atls) : DR Eko Setiawan, Spotyuliana khairiОценок пока нет
- Pneumothorax 180510192017 PDFДокумент27 страницPneumothorax 180510192017 PDFMr AAОценок пока нет
- Chest Tube Insertion: Prepare By: Amrita:Thapa Roll No. 7Документ39 страницChest Tube Insertion: Prepare By: Amrita:Thapa Roll No. 7sushma shresthaОценок пока нет
- Pulmonary SurgeryДокумент18 страницPulmonary SurgeryShy PatelОценок пока нет
- Breathing and Ventilation EmergenciesДокумент13 страницBreathing and Ventilation EmergenciesgosegomangОценок пока нет
- Chest Trauma: Nursing 410 Western Carolina University BSN ProgramДокумент29 страницChest Trauma: Nursing 410 Western Carolina University BSN ProgramShimmering MoonОценок пока нет
- Macro PneumohemoДокумент28 страницMacro PneumohemoSiti AishahОценок пока нет
- Advance Trauma Life Support (ATLS)Документ47 страницAdvance Trauma Life Support (ATLS)Ben Man Jun100% (2)
- Chest PhysiotherapyДокумент61 страницаChest PhysiotherapyAppuОценок пока нет
- Thoracic and Abdominal TraumaДокумент39 страницThoracic and Abdominal TraumaIlliati IbrahimОценок пока нет
- Pneumothorax: - Hitesh Rohit (3 Year B.P.T.)Документ22 страницыPneumothorax: - Hitesh Rohit (3 Year B.P.T.)Hitesh RohitОценок пока нет
- Pneumothorax: - Hitesh Rohit (3 Year B.P.T.)Документ22 страницыPneumothorax: - Hitesh Rohit (3 Year B.P.T.)Hitesh RohitОценок пока нет
- Chest Trauma ManagementДокумент78 страницChest Trauma ManagementHassan Shoukat100% (1)
- Chapter 3Документ54 страницыChapter 3Ayro Business CenterОценок пока нет
- AtelectasisДокумент30 страницAtelectasisashoaib0313Оценок пока нет
- PneumothoraxДокумент30 страницPneumothoraxsanjivdas100% (1)
- Air Way Management (ABCDE of Trauma)Документ25 страницAir Way Management (ABCDE of Trauma)makmmkaОценок пока нет
- Airway and VentilatoryДокумент22 страницыAirway and VentilatoryAbdullah MatarОценок пока нет
- Chest Injury and Its TypesДокумент14 страницChest Injury and Its TypesKoochi PoojithaОценок пока нет
- Cme Trauma Management ZakwanДокумент44 страницыCme Trauma Management ZakwansyasyaОценок пока нет
- Thoracic Decortication: Sabita Chalise Bns 3 YearДокумент32 страницыThoracic Decortication: Sabita Chalise Bns 3 YearRamchandra Chalise100% (1)
- Oxygenation Part 1Документ86 страницOxygenation Part 1Shaira Mae Fangon De GuzmanОценок пока нет
- ArdsДокумент26 страницArdsMarkendey KhannaОценок пока нет
- Respiratory SystemДокумент32 страницыRespiratory SystemvhieeelgbmОценок пока нет
- HematotoraksДокумент15 страницHematotorakssafanj12Оценок пока нет
- Chest TraumaДокумент31 страницаChest Traumawheeyycoldandhot55Оценок пока нет
- Ventilator The Basic CourseДокумент117 страницVentilator The Basic CourseTputrinya FaniddaОценок пока нет
- Chest TraumaДокумент115 страницChest TraumaЕвгений ХанькоОценок пока нет
- Gnrs 5320 Lessonpowerpoint RevisedДокумент30 страницGnrs 5320 Lessonpowerpoint Revisedapi-277849152Оценок пока нет
- The Adult Client With Respiratory Disorder: 2017 EasalavanteДокумент101 страницаThe Adult Client With Respiratory Disorder: 2017 EasalavanteNicholas TagleОценок пока нет
- Trauma Thorax: Disusun Oleh: Uray Ria ApriniДокумент22 страницыTrauma Thorax: Disusun Oleh: Uray Ria ApriniUray RiaОценок пока нет
- Respiratory Physiology Summary NotesДокумент63 страницыRespiratory Physiology Summary NotesAlfredII100% (1)
- SESSION 12 - Tension PneumothoraxДокумент22 страницыSESSION 12 - Tension PneumothoraxLinux KaikaОценок пока нет
- Recognition & Treatment of Pneumothorax Hemothorax, Flail Chest, Stove in ChestДокумент59 страницRecognition & Treatment of Pneumothorax Hemothorax, Flail Chest, Stove in ChestAnusha VergheseОценок пока нет
- Pneumothorax AmierДокумент7 страницPneumothorax Amieramier90Оценок пока нет
- Chest TraumaДокумент175 страницChest TraumaMAMA LALAОценок пока нет
- Respiratory Emergency First AidДокумент13 страницRespiratory Emergency First AidFaithОценок пока нет
- NursingBulletin Notes On PneumothoraxДокумент27 страницNursingBulletin Notes On Pneumothoraxseigelystic100% (11)
- Chapter 13 Student Version The Respiratory System 2020.ppt (1186)Документ18 страницChapter 13 Student Version The Respiratory System 2020.ppt (1186)S. MartinezОценок пока нет
- Chest TraumaДокумент35 страницChest Traumaabu saniОценок пока нет
- Chest TraumaДокумент9 страницChest Traumaapi-3838240100% (7)
- EmpyemaДокумент17 страницEmpyemajismi vallachiraОценок пока нет
- Airway Management: by Paul Edmer CorcueraДокумент40 страницAirway Management: by Paul Edmer CorcueraJeco ValdezОценок пока нет
- CP4. Respiratory SystemДокумент28 страницCP4. Respiratory Systemdafabc50Оценок пока нет
- AirwayДокумент15 страницAirwayYonathan asnakeОценок пока нет
- C.O.P.D: (Chronic Obstructive Pulmonary Disorder)Документ47 страницC.O.P.D: (Chronic Obstructive Pulmonary Disorder)KrystelОценок пока нет
- Respiratory Emergencies: Eileen Humphreys PA-C, EMT-IДокумент71 страницаRespiratory Emergencies: Eileen Humphreys PA-C, EMT-IChristian JaraОценок пока нет
- New Initial Management in TraumaДокумент69 страницNew Initial Management in TraumaAhsan KhanОценок пока нет
- IntubationДокумент41 страницаIntubationNice YouОценок пока нет
- Chest TraumaДокумент23 страницыChest TraumaMutaz DredeiОценок пока нет
- Chest Trauma BCECДокумент25 страницChest Trauma BCECTandin SonamОценок пока нет
- Respiratory NeedsДокумент24 страницыRespiratory NeedsJoyceОценок пока нет
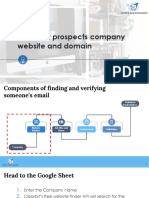
- Find Your Prospects Company Website and DomainДокумент4 страницыFind Your Prospects Company Website and Domaintunde adeniranОценок пока нет
- Financial Literacy - What I Wish I Learned in School - v7Документ213 страницFinancial Literacy - What I Wish I Learned in School - v7tunde adeniranОценок пока нет
- Digital Tools 4SMEsДокумент17 страницDigital Tools 4SMEstunde adeniranОценок пока нет
- Find The Right Prospect's Name at A CompanyДокумент4 страницыFind The Right Prospect's Name at A Companytunde adeniranОценок пока нет
- 8-Entrepreneur Abilities Assessment - AssignmentДокумент1 страница8-Entrepreneur Abilities Assessment - Assignmenttunde adeniranОценок пока нет
- 22-Scientific Reasons To Use ProArgi9Документ2 страницы22-Scientific Reasons To Use ProArgi9tunde adeniranОценок пока нет
- Consulting 993-SampleДокумент48 страницConsulting 993-Sampletunde adeniran100% (1)
- Budget For CDM For May 2009Документ2 страницыBudget For CDM For May 2009tunde adeniranОценок пока нет
- Managing Customers Effectively: by Pharm - Tunde AdeniranДокумент22 страницыManaging Customers Effectively: by Pharm - Tunde Adenirantunde adeniranОценок пока нет
- Corporate I-Bank: Application FormДокумент4 страницыCorporate I-Bank: Application Formtunde adeniranОценок пока нет
- My Coupon DetailsДокумент2 страницыMy Coupon Detailstunde adeniranОценок пока нет
- CDM Training Lagos 2009Документ1 страницаCDM Training Lagos 2009tunde adeniranОценок пока нет
- Design BriefДокумент1 страницаDesign Brieftunde adeniranОценок пока нет
- For The Free Video Please SeeДокумент5 страницFor The Free Video Please Seetunde adeniranОценок пока нет
- Moisture and Total Solids AnalysisДокумент44 страницыMoisture and Total Solids AnalysisNicholas BoampongОценок пока нет
- AssignmentДокумент13 страницAssignmentSwakshar DebОценок пока нет
- Ceu Guidance Problematic Bleeding Hormonal ContraceptionДокумент28 страницCeu Guidance Problematic Bleeding Hormonal Contraceptionmarina_shawkyОценок пока нет
- Brainedema 160314142234Документ39 страницBrainedema 160314142234Lulu LuwiiОценок пока нет
- South Valley University Faculty of Science Geology Department Dr. Mohamed Youssef AliДокумент29 страницSouth Valley University Faculty of Science Geology Department Dr. Mohamed Youssef AliHari Dante Cry100% (1)
- PANCREATITISДокумент38 страницPANCREATITISVEDHIKAVIJAYANОценок пока нет
- Hazel Rhs Horticulture Level 2 Essay 1Документ24 страницыHazel Rhs Horticulture Level 2 Essay 1hazeldwyerОценок пока нет
- Soccer Training DiaryДокумент1 страницаSoccer Training DiaryMark DeaconОценок пока нет
- Famous Bombers of The Second World War - 1st SeriesДокумент142 страницыFamous Bombers of The Second World War - 1st Seriesgunfighter29100% (1)
- 3rd Stage ComplicationsДокумент84 страницы3rd Stage ComplicationsDream100% (1)
- Pediatric Gynecology BaruДокумент79 страницPediatric Gynecology BaruJosephine Irena100% (2)
- 1.1 Introduction To KennametalДокумент40 страниц1.1 Introduction To KennametalVig PankajОценок пока нет
- 4MA0 4H MSC 20140306Документ14 страниц4MA0 4H MSC 20140306HaiqaPervezОценок пока нет
- Manual de Electronica HardbookДокумент970 страницManual de Electronica HardbookninoferОценок пока нет
- Nitrogen CycleДокумент12 страницNitrogen Cycleasa bspcpkОценок пока нет
- The Common Reader-Virginia WoolfДокумент216 страницThe Common Reader-Virginia WoolfRusudan VardiashviliОценок пока нет
- Faithgirlz Handbook, Updated and ExpandedДокумент15 страницFaithgirlz Handbook, Updated and ExpandedFaithgirlz75% (4)
- Library: Astrology and WisdomДокумент13 страницLibrary: Astrology and Wisdomalimuhammedkhan2115Оценок пока нет
- Fo Transfer ProcedureДокумент8 страницFo Transfer ProcedureadityasahayОценок пока нет
- Classical Feedback Control With MATLAB - Boris J. Lurie and Paul J. EnrightДокумент477 страницClassical Feedback Control With MATLAB - Boris J. Lurie and Paul J. Enrightffranquiz100% (2)
- 11 - Morphology AlgorithmsДокумент60 страниц11 - Morphology AlgorithmsFahad MattooОценок пока нет
- Wiring of The Distribution Board With RCD (Residual Current Devices) - Single Phase Home SupplyДокумент14 страницWiring of The Distribution Board With RCD (Residual Current Devices) - Single Phase Home SupplyKadhir BoseОценок пока нет
- Geology of Johannesburg ReadingДокумент2 страницыGeology of Johannesburg ReadingKavish DayaОценок пока нет
- Initiation in Pre-Tantrasamuccaya Kerala Tantric Literature PDFДокумент24 страницыInitiation in Pre-Tantrasamuccaya Kerala Tantric Literature PDFVenkateswaran NarayananОценок пока нет
- IMCI UpdatedДокумент5 страницIMCI UpdatedMalak RagehОценок пока нет
- JDM B18C Type RДокумент6 страницJDM B18C Type RSeenka CapuqОценок пока нет
- Theory of Earth's Magnetism and It's Relation ToДокумент15 страницTheory of Earth's Magnetism and It's Relation ToMaster Irvin100% (1)
- TXN Alarms 18022014Документ12 страницTXN Alarms 18022014Sid GrgОценок пока нет
- Defect Origin (J) Phase Requirement Analysis Design Coding Unit TestingДокумент87 страницDefect Origin (J) Phase Requirement Analysis Design Coding Unit Testingashish_jain_csОценок пока нет