Вам также может понравиться
- MKSAP 17 Endocrinology and Metabolism PDFДокумент155 страницMKSAP 17 Endocrinology and Metabolism PDFAkhil Bansal75% (4)
- Uti CPG PPSДокумент6 страницUti CPG PPSPernel Jose Alam Micubo100% (1)
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtОт EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtРейтинг: 5 из 5 звезд5/5 (1)
- Valvular Heart Disease Medical Surgical NursingДокумент75 страницValvular Heart Disease Medical Surgical NursingGodfrey Franco88% (8)
- Congenital Heart DiseaseДокумент22 страницыCongenital Heart DiseaseDiosa MedinaОценок пока нет
- Pathophysiology Congenital Heart Disease-1Документ54 страницыPathophysiology Congenital Heart Disease-1single_ladyОценок пока нет
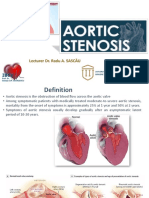
- Aortic Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Internal Medicine (P-A) Chattogram Medical CollegeДокумент13 страницAortic Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Internal Medicine (P-A) Chattogram Medical CollegeAsrafur RahmanОценок пока нет
- Valvular & Inflammatory HDДокумент33 страницыValvular & Inflammatory HDSinam SinghaОценок пока нет
- ucu-CHDs 240114 230618Документ68 страницucu-CHDs 240114 230618BrianОценок пока нет
- Atrial Septial DefectДокумент22 страницыAtrial Septial DefectJulie MckinneyОценок пока нет
- Congenital Heart DiseasesДокумент121 страницаCongenital Heart DiseasesJayvee V. De GuzmanОценок пока нет
- Congenital Heart DiseasesДокумент27 страницCongenital Heart DiseasesJumar ValdezОценок пока нет
- Tetralogy of FallotДокумент31 страницаTetralogy of FallotDevipriya MajumderОценок пока нет
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingДокумент69 страницUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingErica Veluz LuyunОценок пока нет
- CHD - Med IIДокумент70 страницCHD - Med IISanskruthi KurniОценок пока нет
- Congenital Heart DiseaseДокумент57 страницCongenital Heart DiseaseAparna RawatОценок пока нет
- Ventricular Septal Defects: Drmlpatel Department of Medicine KgmuДокумент19 страницVentricular Septal Defects: Drmlpatel Department of Medicine KgmuDurgesh PushkarОценок пока нет
- Coarctation of The Aorta.: Franz Fanon University Medical Faculty 2020 June Peds. LessonДокумент12 страницCoarctation of The Aorta.: Franz Fanon University Medical Faculty 2020 June Peds. LessongibreilОценок пока нет
- K7 - Supraventricular Tachycardia (SVT)Документ44 страницыK7 - Supraventricular Tachycardia (SVT)Zikri Putra Lan LubisОценок пока нет
- Cyanotic Heart DiseaseДокумент66 страницCyanotic Heart DiseasePrasanth SankarОценок пока нет
- Case Scenerio: DR Sourath Munir Malkani Fcps-Ii TraineДокумент31 страницаCase Scenerio: DR Sourath Munir Malkani Fcps-Ii TraineSoonh ChannaОценок пока нет
- CTSU Presentation PDAДокумент41 страницаCTSU Presentation PDAEdwin OkonОценок пока нет
- Acyanotic CHD 2008Документ50 страницAcyanotic CHD 2008Ana Abadi Al IndОценок пока нет
- Congenital Heart DiseaseДокумент135 страницCongenital Heart DiseaseMahmudahОценок пока нет
- Congenital Heart Disease - Part IДокумент95 страницCongenital Heart Disease - Part IMeraol HusseinОценок пока нет
- Adult CHD 2015Документ42 страницыAdult CHD 2015Pshtiwan MahmoodОценок пока нет
- Congenital Disorder ASD VSDДокумент50 страницCongenital Disorder ASD VSDSachin DwivediОценок пока нет
- Aortic Regurgitation by DR DilmoДокумент37 страницAortic Regurgitation by DR Dilmosinan kОценок пока нет
- Cardio-Respiratory Conditions: by DR Priscus MushiДокумент73 страницыCardio-Respiratory Conditions: by DR Priscus MushiMusaОценок пока нет
- #5 Neonatal Cardiac AnomaliesДокумент93 страницы#5 Neonatal Cardiac AnomaliesSittie Hania100% (2)
- Congenital Heart DefectsДокумент73 страницыCongenital Heart DefectsStaen KisОценок пока нет
- Congenital Heart Disease: Kriti Puri, MD Hugh D. Allen, MD Athar M. Qureshi, MDДокумент30 страницCongenital Heart Disease: Kriti Puri, MD Hugh D. Allen, MD Athar M. Qureshi, MDhari ilman toniОценок пока нет
- Odia Tetralogy of FallotДокумент25 страницOdia Tetralogy of Fallotvictorjonathan567Оценок пока нет
- Congenital Heart Disease: Thoracic Conference Frank Nami, M.DДокумент49 страницCongenital Heart Disease: Thoracic Conference Frank Nami, M.DMarie CrystallineОценок пока нет
- Congenital Heart Disease: Eu MBCHB 4Документ66 страницCongenital Heart Disease: Eu MBCHB 4Malueth AnguiОценок пока нет
- 4.3.aortic StenosisДокумент61 страница4.3.aortic StenosisMuh BluОценок пока нет
- Cardiovascular Diseases VSD Asd 2022 1Документ16 страницCardiovascular Diseases VSD Asd 2022 1Boyu GrtrОценок пока нет
- Hypertrophic Cardiomyopathy: Joisy Aloor Leonard Shaju Smit Bhaisare Shawn RyneДокумент36 страницHypertrophic Cardiomyopathy: Joisy Aloor Leonard Shaju Smit Bhaisare Shawn RyneJoisy Aloor100% (1)
- Pediatric Heart FailureДокумент34 страницыPediatric Heart FailuretoyyibОценок пока нет
- Congenital Heart Disorders (Acyanotic)Документ53 страницыCongenital Heart Disorders (Acyanotic)Hannah LaputОценок пока нет
- Congenital Heart DiseaseДокумент77 страницCongenital Heart DiseaseMalueth Angui100% (1)
- Aortic StenosisДокумент17 страницAortic StenosisManjunatha HR100% (1)
- CVD 10 (١) PDFДокумент23 страницыCVD 10 (١) PDFHmhm HmhmОценок пока нет
- Atrial Septal Defects (ASD)Документ30 страницAtrial Septal Defects (ASD)wissam salimОценок пока нет
- Department of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Документ51 страницаDepartment of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Suba Saravanan 12Оценок пока нет
- Cardio My Opa ThiesДокумент73 страницыCardio My Opa Thiesriyazadsumaiyajb2003Оценок пока нет
- Lec 2, Congenital Heart DiseasesДокумент61 страницаLec 2, Congenital Heart DiseasesAlexandrescuОценок пока нет
- Acynotic Heart DiseasesДокумент13 страницAcynotic Heart DiseasesSimran JosanОценок пока нет
- Congenital Heart Disease: Hema Rajendran B.SC (N) NICU Staff NurseДокумент23 страницыCongenital Heart Disease: Hema Rajendran B.SC (N) NICU Staff NurseddОценок пока нет
- Valvular Heart DiseasesДокумент60 страницValvular Heart DiseasesEthiopia TekdemОценок пока нет
- Atrial Septal DefectsДокумент24 страницыAtrial Septal DefectsSaiaDaphiОценок пока нет
- Tricuspid Atresia VivekДокумент66 страницTricuspid Atresia VivekIlham FatthurОценок пока нет
- 23 May 2011 Peerapat Thaisiam Yossavadee RuamcharoenДокумент109 страниц23 May 2011 Peerapat Thaisiam Yossavadee RuamcharoenRapid MedicineОценок пока нет
- MURMURДокумент21 страницаMURMURtoyyibОценок пока нет
- Congenital Heart Diseases Practical Approach in Children With Heart MurmurДокумент51 страницаCongenital Heart Diseases Practical Approach in Children With Heart Murmurdennyyy175Оценок пока нет
- Valvular Heart DiseaseДокумент66 страницValvular Heart DiseaseRita LakhaniОценок пока нет
- Pastest Note 5Документ4 страницыPastest Note 5Amer AldhaliaОценок пока нет
- Aortic Stenosis:: Updates in Diagnosis & ManagementДокумент48 страницAortic Stenosis:: Updates in Diagnosis & ManagementCuca PcelaОценок пока нет
- Acyanotic CHDДокумент83 страницыAcyanotic CHDmrinmayee deshmukhОценок пока нет
- CardiologyДокумент43 страницыCardiologyhasanatiya41Оценок пока нет
- Surgical and Post-Operative ManagementДокумент6 страницSurgical and Post-Operative ManagementPernel Jose Alam MicuboОценок пока нет
- Periodic Health ExamДокумент23 страницыPeriodic Health ExamPernel Jose Alam MicuboОценок пока нет
- ASD Internship ReportingДокумент14 страницASD Internship ReportingPernel Jose Alam MicuboОценок пока нет
- Peptic Ulcer DiseaseДокумент14 страницPeptic Ulcer DiseasePernel Jose Alam MicuboОценок пока нет
- Acute Kidney Injury: 2017 A D R V 1: C K DДокумент31 страницаAcute Kidney Injury: 2017 A D R V 1: C K DPernel Jose Alam MicuboОценок пока нет
- Tension Type Headache and EncephalitisДокумент11 страницTension Type Headache and EncephalitisPernel Jose Alam MicuboОценок пока нет
- Pathophysiology of Tetanus: Precipitating Factors: Predisposing FactorsДокумент2 страницыPathophysiology of Tetanus: Precipitating Factors: Predisposing FactorsPernel Jose Alam Micubo100% (1)
- UTI - Internship PresentationДокумент27 страницUTI - Internship PresentationPernel Jose Alam MicuboОценок пока нет
- Day Rule in Rule OutДокумент5 страницDay Rule in Rule OutPernel Jose Alam MicuboОценок пока нет
- Adulthood & Geriatric PsychiatryДокумент13 страницAdulthood & Geriatric PsychiatryPernel Jose Alam MicuboОценок пока нет
- VertebraeДокумент8 страницVertebraePernel Jose Alam MicuboОценок пока нет
- Management of Acute MI, Role of Streptokinase, NicvdДокумент22 страницыManagement of Acute MI, Role of Streptokinase, NicvdNavojit ChowdhuryОценок пока нет
- Sodium Glucose Cotransporter-2 Inhibition For Acute Myocardial InfarctionДокумент11 страницSodium Glucose Cotransporter-2 Inhibition For Acute Myocardial InfarctionmedicabrujaОценок пока нет
- Guidelines On Sports Cardiology and - ExerciseДокумент80 страницGuidelines On Sports Cardiology and - ExerciseBruno S. Homem De FariaОценок пока нет
- Management of Acute Kidney Injury in Children: Sri Lanka Journal of Child Health January 2019Документ6 страницManagement of Acute Kidney Injury in Children: Sri Lanka Journal of Child Health January 2019HannaSaskiaIIОценок пока нет
- Chapter 10 CardiovascularДокумент3 страницыChapter 10 CardiovascularBernard Paul Guinto100% (1)
- Erythema Marginatum Chorea: Migratory Polyarthritis Cardiac Involvement Subcutaneous NodulesДокумент27 страницErythema Marginatum Chorea: Migratory Polyarthritis Cardiac Involvement Subcutaneous NodulesMisbah KaleemОценок пока нет
- 4 U1.0 B978 0 323 05611 3..00012 4..DOCPDFДокумент97 страниц4 U1.0 B978 0 323 05611 3..00012 4..DOCPDFmisstina.19876007Оценок пока нет
- Ton Mitral Valve ReplacementДокумент3 страницыTon Mitral Valve ReplacementSony TonОценок пока нет
- ACLS Official GuideДокумент11 страницACLS Official GuideICU RSPGОценок пока нет
- Open Heart SurgeryДокумент11 страницOpen Heart SurgeryFlavia Sz100% (2)
- Management Algorithm For Adult With HyperkalemiaДокумент1 страницаManagement Algorithm For Adult With HyperkalemiaAnjiОценок пока нет
- 45 Tahun Dengan Manifestasi Stokes-Adams Attack: Laporan KasusДокумент7 страниц45 Tahun Dengan Manifestasi Stokes-Adams Attack: Laporan KasusKena BenОценок пока нет
- Basic EP 01Документ53 страницыBasic EP 01Hany100% (2)
- Ecg 01Документ103 страницыEcg 01Bandar al ghamdi100% (1)
- Acute and Chronic Renal Failure Student 2013Документ76 страницAcute and Chronic Renal Failure Student 2013phoenix180100% (1)
- Atrial FibrillationДокумент20 страницAtrial Fibrillationjack sawdaОценок пока нет
- PcicardДокумент2 страницыPcicardWahdat100% (1)
- Lippincott Antiarrhythmics 7Документ2 страницыLippincott Antiarrhythmics 7Wijdan HatemОценок пока нет
- The Dandenong Dossier 2010Документ243 страницыThe Dandenong Dossier 2010reshminОценок пока нет
- 10 Besar Penyakit Rawat Inap & 10 Besar Tindakan Rawat InapДокумент1 страница10 Besar Penyakit Rawat Inap & 10 Besar Tindakan Rawat InapPendaftaran MCUОценок пока нет
- TurkJEmergMed22275 5543957 - 013223 2Документ8 страницTurkJEmergMed22275 5543957 - 013223 2Ria Junita AyuОценок пока нет
- Renal Learning OutcomesДокумент11 страницRenal Learning OutcomesBhuwan TandonОценок пока нет
- Cardiac QuestionsДокумент13 страницCardiac Questionsacque100% (1)
- NCP Heart FailureДокумент2 страницыNCP Heart FailureDayan Cabriga100% (1)
- Reglas de ChamberlainДокумент33 страницыReglas de ChamberlainFran Burga Becerra100% (1)
- Cardiovascular Drugs XL ChartДокумент4 страницыCardiovascular Drugs XL Chartcdp158767% (3)
- Consensus From The 10th European Bifurcation Club MeetingДокумент16 страницConsensus From The 10th European Bifurcation Club MeetingMichael Jansen SulaimanОценок пока нет
- Heart Failure: More... 58Документ4 страницыHeart Failure: More... 58pmОценок пока нет
- ACLSДокумент61 страницаACLSmgthida935100% (1)