Вам также может понравиться
- Freedom Alliance - About Us Page 10f2Документ132 страницыFreedom Alliance - About Us Page 10f2CREWОценок пока нет
- Financial Environment (Markets, Institutions & Interest Rate)Документ20 страницFinancial Environment (Markets, Institutions & Interest Rate)Umer ShaikhОценок пока нет
- DFIA - Worksheet in Cultural Mapping (Formatted - Submitted)Документ16 страницDFIA - Worksheet in Cultural Mapping (Formatted - Submitted)franzОценок пока нет
- Professional Adjustment (Week 4)Документ19 страницProfessional Adjustment (Week 4)joeljohndelamercedОценок пока нет
- Medoc CompanyДокумент8 страницMedoc CompanyGaneshОценок пока нет
- Over A Century of Capital Market History Measuring Portfolio Risk Calculating Portfolio Risk Beta and Unique Risk Diversification & Value AdditivityДокумент48 страницOver A Century of Capital Market History Measuring Portfolio Risk Calculating Portfolio Risk Beta and Unique Risk Diversification & Value AdditivityanushreegoОценок пока нет
- Chapter1 Slides FIN 4354Документ14 страницChapter1 Slides FIN 4354Shakkhor ChowdhuryОценок пока нет
- Return & RiskДокумент17 страницReturn & RiskMonoar HossainОценок пока нет
- Financial Markets and InstrumentsДокумент2 страницыFinancial Markets and InstrumentsKristel SumabatОценок пока нет
- NSTP 2D Decision MakingДокумент29 страницNSTP 2D Decision MakingJulius Memeg Panayo0% (2)
- Promotion, TransferДокумент17 страницPromotion, TransferShipra Srivastava100% (1)
- Financial Markets and IntermediariesДокумент3 страницыFinancial Markets and IntermediariesAnonymous tiMNO7VОценок пока нет
- Chapter 6 Risk and Return LectureДокумент10 страницChapter 6 Risk and Return LectureAia GarciaОценок пока нет
- 30 Golden Rules of Successful Restaurant OperationДокумент2 страницы30 Golden Rules of Successful Restaurant OperationInês Serra BrandãoОценок пока нет
- Vendor Obligations and Warranties in Sales ContractsДокумент18 страницVendor Obligations and Warranties in Sales ContractsKaren Africano100% (1)
- Chapter 16 Planning The Firm's Financing MixДокумент12 страницChapter 16 Planning The Firm's Financing MixAia Garcia50% (2)
- Basic Economic QuestionsДокумент6 страницBasic Economic Questionsnusrat1998Оценок пока нет
- Chapter 08 Risk and Rates of ReturnДокумент48 страницChapter 08 Risk and Rates of ReturnNaida's StuffОценок пока нет
- Sublimation and Melting Point DeterminationДокумент2 страницыSublimation and Melting Point DeterminationEdlock HolmesОценок пока нет
- Lecture 2. Financial Markets, Institutions and Interest RatesДокумент28 страницLecture 2. Financial Markets, Institutions and Interest RatesmuhammadnaumairОценок пока нет
- Crime Investigation Plan Guide - SMECAC Principles, Evidence Matrix, Resource SheetДокумент189 страницCrime Investigation Plan Guide - SMECAC Principles, Evidence Matrix, Resource SheetAbdul Aziz Akil RiasОценок пока нет
- Interest RatesДокумент11 страницInterest RatesPau GigantoneОценок пока нет
- CE 446-Assignment 1Документ2 страницыCE 446-Assignment 1Renzo Rufin PoliñoОценок пока нет
- Youth Participation in Politics in CambodiaДокумент23 страницыYouth Participation in Politics in CambodiaEd SawyerОценок пока нет
- July 10, 2019 Lesson Interest RateДокумент33 страницыJuly 10, 2019 Lesson Interest RateMarkus Bernabe DaviraОценок пока нет
- 1 Introduction To Management and OrganizationsДокумент40 страниц1 Introduction To Management and OrganizationsZiko2billionОценок пока нет
- Wilson Reyes Jr Construction Scheduling ResumeДокумент5 страницWilson Reyes Jr Construction Scheduling ResumeMichelle de GuzmanОценок пока нет
- Judicial Choice of Law in Haag vs. BarnesДокумент2 страницыJudicial Choice of Law in Haag vs. BarnesFishcaОценок пока нет
- Chapter 17 Dividend PolicyДокумент7 страницChapter 17 Dividend PolicyAia GarciaОценок пока нет
- Right To Life Movement PowerpointДокумент8 страницRight To Life Movement Powerpointapi-452788589Оценок пока нет
- Firstsem Sales EditedДокумент43 страницыFirstsem Sales EditedjohnisflyОценок пока нет
- Theories of International Trade and InvestmentДокумент16 страницTheories of International Trade and InvestmentSapna KumariОценок пока нет
- Breast FeedingДокумент18 страницBreast FeedingAnis Rakhmawati100% (1)
- I Am A Dominican!: FaithДокумент22 страницыI Am A Dominican!: FaithWilliam Soneja Calapini100% (1)
- Pig Heart Dissection Lab 2012-2013 Fist UnicornДокумент19 страницPig Heart Dissection Lab 2012-2013 Fist Unicornapi-169772897Оценок пока нет
- Function of Financial MarketsДокумент11 страницFunction of Financial MarketsYepuru ChaithanyaОценок пока нет
- CAPM: Capital Asset Pricing Model ExplainedДокумент43 страницыCAPM: Capital Asset Pricing Model ExplainedProf.V.Vanaja sureshОценок пока нет
- Demetria vs. AlbaДокумент3 страницыDemetria vs. AlbaShayrie WynneОценок пока нет
- Capm 1 PDFДокумент8 страницCapm 1 PDFAbhishek AroraОценок пока нет
- FMДокумент36 страницFMJenelle ReyesОценок пока нет
- 34 Philippine Airlines, Inc. vs. Savillo, G.R. No. 149547 PDFДокумент12 страниц34 Philippine Airlines, Inc. vs. Savillo, G.R. No. 149547 PDFpa0l0sОценок пока нет
- Introduction To PathophysiologyДокумент29 страницIntroduction To PathophysiologystevencongressОценок пока нет
- Golden Rice Genetic PresentationДокумент23 страницыGolden Rice Genetic PresentationPeter FadoulОценок пока нет
- Trisomy 21-Down SyndromeДокумент1 страницаTrisomy 21-Down Syndromeapi-253727022Оценок пока нет
- Chapter 3 Bond Duration and Bond PricingДокумент28 страницChapter 3 Bond Duration and Bond PricingClaire VensueloОценок пока нет
- #4 Pas 8Документ3 страницы#4 Pas 8Shara Joy B. Parayno100% (1)
- Chapter Exercises Risk & ReturnДокумент5 страницChapter Exercises Risk & ReturnEvelyn LeeОценок пока нет
- ANATOMY AND PHYSIOLOGY REVIEW QUESTIONSДокумент15 страницANATOMY AND PHYSIOLOGY REVIEW QUESTIONSMarcoОценок пока нет
- Economic and Political Changes in Occupied PhilippinesДокумент2 страницыEconomic and Political Changes in Occupied Philippinesbam11219067% (3)
- Fetal Positions and Presentations GuideДокумент11 страницFetal Positions and Presentations GuideShanon France100% (1)
- Lecture Rickettsia Chlamydia, MycoplasmaДокумент49 страницLecture Rickettsia Chlamydia, MycoplasmaHabeeb Ali Baig100% (3)
- Should A Country Adopt Fixed or Flexible Exchange Rate System?Документ8 страницShould A Country Adopt Fixed or Flexible Exchange Rate System?Zakaria CassimОценок пока нет
- The Miracle of LifeДокумент6 страницThe Miracle of LifeKiseKunОценок пока нет
- Hispath NotesДокумент9 страницHispath NotesFait HeeОценок пока нет
- Factors Affecting LaborДокумент2 страницыFactors Affecting LaborChristina Richards100% (1)
- Nursing Process For A Client With Molar Pregnancy (H-Mole)Документ24 страницыNursing Process For A Client With Molar Pregnancy (H-Mole)api-370148995% (19)
- Uterine ProlapseДокумент44 страницыUterine ProlapseMoi Mendoza83% (6)
- Nursing Molar PregnancyДокумент24 страницыNursing Molar PregnancyLord Pozak Miller100% (1)
- Ectopic Pregnancy 1Документ25 страницEctopic Pregnancy 1eightОценок пока нет
- RR 3Документ9 страницRR 3Olivelhynn BernaldoОценок пока нет
- Asa Physical Status Classification SystemДокумент4 страницыAsa Physical Status Classification SystemOlivelhynn BernaldoОценок пока нет
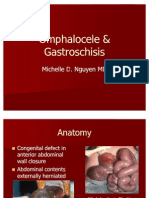
- Omphalocele GastroschisisДокумент12 страницOmphalocele GastroschisisOlivelhynn Bernaldo100% (1)
- Chronic Obstructive Pulmonary DisorderДокумент11 страницChronic Obstructive Pulmonary DisorderOlivelhynn BernaldoОценок пока нет
- Pathophysiology Diagram of Congestive Heart FailureДокумент3 страницыPathophysiology Diagram of Congestive Heart Failurea_samiane64% (11)
- General Data and Nursing Care Plan for a 1 Month Old Male Patient with PneumoniaДокумент10 страницGeneral Data and Nursing Care Plan for a 1 Month Old Male Patient with PneumoniaOlivelhynn BernaldoОценок пока нет
- Sexuality and Sexual Expression Throughout LifeДокумент25 страницSexuality and Sexual Expression Throughout LifeOlivelhynn Bernaldo100% (1)
- Evaluasi Program Pemberian Tablet Tambah Darah Pada Remaja Putri Anemia Dan Non Anemia Di Wilayah Puskesmas AntapaniДокумент9 страницEvaluasi Program Pemberian Tablet Tambah Darah Pada Remaja Putri Anemia Dan Non Anemia Di Wilayah Puskesmas AntapaniAgung JayaОценок пока нет
- Unit Vii Assessment of The Abdomen, Anus and RectumДокумент86 страницUnit Vii Assessment of The Abdomen, Anus and Rectumramzan aliОценок пока нет
- Vascular Abnormalities of SSCДокумент9 страницVascular Abnormalities of SSCCristina ElenaОценок пока нет
- MAKALAH. Memahami Dasar Anatomi Tubuh ManusiaДокумент19 страницMAKALAH. Memahami Dasar Anatomi Tubuh ManusiadediОценок пока нет
- Biologie - Funcția de NutrițieДокумент23 страницыBiologie - Funcția de NutrițieDaria MargaritОценок пока нет
- Solution Brahmastra-19-02-2023Документ38 страницSolution Brahmastra-19-02-2023Vaibhav Kumar SinghОценок пока нет
- Basic and Bedside ElectrocardiographyДокумент464 страницыBasic and Bedside ElectrocardiographyBimo Panji Kumoro100% (2)
- 72 Hours Chick EmbryoДокумент18 страниц72 Hours Chick EmbryoZhairra Marie DionsonОценок пока нет
- Cranial Nerve: Dr. Dian Prasetyo Wibisono, M.SCДокумент49 страницCranial Nerve: Dr. Dian Prasetyo Wibisono, M.SCgeneОценок пока нет
- The Lympho Glandular and Intugmentary System: Presenter: Abdurke Dido - Physician (MD) May 22,2011Документ62 страницыThe Lympho Glandular and Intugmentary System: Presenter: Abdurke Dido - Physician (MD) May 22,2011Worku KifleОценок пока нет
- Stem Cell Therapy in Heart Diseases - Cell Types, Mechanisms and Improvement StrategiesДокумент49 страницStem Cell Therapy in Heart Diseases - Cell Types, Mechanisms and Improvement StrategiesDana LebadaОценок пока нет
- Skills # 8: THE ABDOMEN: Procedure Rationale CXNRДокумент3 страницыSkills # 8: THE ABDOMEN: Procedure Rationale CXNRAlyssa Ashley A. ImamОценок пока нет
- Extensor Indicis Brevis: An Unusual Muscular VariantДокумент3 страницыExtensor Indicis Brevis: An Unusual Muscular VariantMichele GonçalvesОценок пока нет
- Atlas Animal Anatomy For ArtistsДокумент155 страницAtlas Animal Anatomy For Artistsdefkacko100% (2)
- 4 BoardCompanion BiologyДокумент58 страниц4 BoardCompanion BiologyEntirety 4uОценок пока нет
- Visual System QuizДокумент27 страницVisual System QuizTEOFILO PALSIMON JR.Оценок пока нет
- Q1 W5 PE 11 Managing Stress Through PhysicalДокумент6 страницQ1 W5 PE 11 Managing Stress Through PhysicalJulie Ann Suarez0% (1)
- Cyclosporine HyperkalemiaДокумент5 страницCyclosporine HyperkalemiaAlba RosesОценок пока нет
- Importance of SleepДокумент10 страницImportance of SleepKopano'Gucci'ModisenyaneОценок пока нет
- CarolinaManyariDiaz CVДокумент2 страницыCarolinaManyariDiaz CVJONATHAN CORDOVAОценок пока нет
- Anatomia FacialДокумент10 страницAnatomia FacialIgor NatanyoОценок пока нет
- Biosynthesis of CholesterolДокумент20 страницBiosynthesis of CholesterolAboubakar Moalim Mahad moh'dОценок пока нет
- Farmasetika II - AnalgetikДокумент15 страницFarmasetika II - AnalgetikNur FitriОценок пока нет
- 0 BooksДокумент20 страниц0 Bookslaraib zahidОценок пока нет
- Concept Strengthening Sheet (CSS-01) Based On CST-01 & 02 - ZoologyДокумент4 страницыConcept Strengthening Sheet (CSS-01) Based On CST-01 & 02 - ZoologyUdithyaОценок пока нет
- You Can't Take It With You - Straight Talk About Epigenetics and Intergenerational TraumaДокумент17 страницYou Can't Take It With You - Straight Talk About Epigenetics and Intergenerational TraumaArindam ChakrabortyОценок пока нет
- 0710 Biology Past Questions From June 2000 To June 2021Документ46 страниц0710 Biology Past Questions From June 2000 To June 2021Stella DjuikomОценок пока нет
- Last Look PathologyДокумент136 страницLast Look Pathologyrama100% (1)
- Cell, Basic Structure of All Living Creatures: Life Science, Human BiologyДокумент11 страницCell, Basic Structure of All Living Creatures: Life Science, Human BiologyAshleigh Jenson WilliamsonОценок пока нет
- Fluids: Drip ChamberДокумент5 страницFluids: Drip ChamberMacen OrtegaОценок пока нет