Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Africanas Journal Volume 3 No. 2Документ102 страницыAfricanas Journal Volume 3 No. 2Gordon-Conwell Theological Seminary100% (2)
- Neoreviews: Moc MocДокумент76 страницNeoreviews: Moc Mocsalamred100% (2)
- Plate Tectonics QuizДокумент6 страницPlate Tectonics QuizJordan Santos100% (1)
- Lab Report: SimulinkДокумент2 страницыLab Report: SimulinkM Luqman FarooquiОценок пока нет
- Acid Base AnswersДокумент4 страницыAcid Base Answersapi-232466940Оценок пока нет
- People Vs GonaДокумент2 страницыPeople Vs GonaM Azeneth JJ100% (1)
- Swimming Pool - PWTAG CodeofPractice1.13v5 - 000Документ58 страницSwimming Pool - PWTAG CodeofPractice1.13v5 - 000Vin BdsОценок пока нет
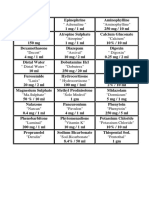
- أدوية الطوارىءДокумент162 страницыأدوية الطوارىءManar22Оценок пока нет
- F A T City Workshop NotesДокумент3 страницыF A T City Workshop Notesapi-295119035Оценок пока нет
- I. Purpose: Clinical Practice Policy: Effective DateДокумент7 страницI. Purpose: Clinical Practice Policy: Effective DatesalamredОценок пока нет
- The Role of Chest X-Ray in Monitoring The Lung Changes Among Covid-19 Patients in Gaza StripДокумент31 страницаThe Role of Chest X-Ray in Monitoring The Lung Changes Among Covid-19 Patients in Gaza StripsalamredОценок пока нет
- Respiratory Distress Syndrome Management in Resource Limited Settings-Current Evidence and Opportunities in 2022Документ15 страницRespiratory Distress Syndrome Management in Resource Limited Settings-Current Evidence and Opportunities in 2022salamredОценок пока нет
- Pgmee Test Series For Neet & Aiims: WWW - Aim4Aiims - In/Pg +91-7529938911Документ74 страницыPgmee Test Series For Neet & Aiims: WWW - Aim4Aiims - In/Pg +91-7529938911salamredОценок пока нет
- RPA Newborn Care Guidelines: Royal Prince Alfred Hospital Umbilical Venous CatheterisationДокумент16 страницRPA Newborn Care Guidelines: Royal Prince Alfred Hospital Umbilical Venous CatheterisationsalamredОценок пока нет
- Clinical Audit On Healthcare Provider Hand Hygiene at Neonatal ICU of EL-Helal EL-Emarati HospitalДокумент43 страницыClinical Audit On Healthcare Provider Hand Hygiene at Neonatal ICU of EL-Helal EL-Emarati HospitalsalamredОценок пока нет
- Slides Accompanying Training Films: To Use in Education Sessions For Trainers, Observers and Health-Care WorkersДокумент47 страницSlides Accompanying Training Films: To Use in Education Sessions For Trainers, Observers and Health-Care WorkerssalamredОценок пока нет
- Clinical Final ExamДокумент7 страницClinical Final ExamsalamredОценок пока нет
- AAA Guidelines 2011 PDFДокумент78 страницAAA Guidelines 2011 PDFsalamredОценок пока нет
- Respiratory Distress in Newborn: Presented By: Dr. Walaa MousaДокумент74 страницыRespiratory Distress in Newborn: Presented By: Dr. Walaa MousasalamredОценок пока нет
- Family Medicine Part One Exam Blueprint 2018Документ4 страницыFamily Medicine Part One Exam Blueprint 2018salamredОценок пока нет
- Clinical Final ExamДокумент7 страницClinical Final ExamsalamredОценок пока нет
- ERC Summary Booklet HRESДокумент24 страницыERC Summary Booklet HRESatika ichaОценок пока нет
- Chest XrayДокумент13 страницChest XrayMohamed Abo SeifОценок пока нет
- Newborn and Infant Hearing Screening ReportДокумент39 страницNewborn and Infant Hearing Screening ReportAdityaHudiansyahОценок пока нет
- Talking About Coronavirus 19 With Young ChildrenДокумент10 страницTalking About Coronavirus 19 With Young ChildrensalamredОценок пока нет
- 2019 Ncov FactsheetДокумент1 страница2019 Ncov FactsheetskarthiphdОценок пока нет
- AminophyllineДокумент3 страницыAminophyllinesalamredОценок пока нет
- Coronavirus and Power. Impact On International PoliticsДокумент4 страницыCoronavirus and Power. Impact On International PoliticsveroОценок пока нет
- Sublingual Morphine: Efficacy Reviewed: Review ArticleДокумент9 страницSublingual Morphine: Efficacy Reviewed: Review ArticlesalamredОценок пока нет
- Perinatal/Neonatal CasebookДокумент4 страницыPerinatal/Neonatal CasebooksalamredОценок пока нет
- DM DrugsДокумент1 страницаDM DrugssalamredОценок пока нет
- Developmental Enamel Defects in Primary DentitionДокумент8 страницDevelopmental Enamel Defects in Primary DentitionAndrea LawОценок пока нет
- Respiratory DistressДокумент39 страницRespiratory DistresssalamredОценок пока нет
- Respiratory Distress NBДокумент63 страницыRespiratory Distress NBsalamredОценок пока нет
- Paeds IV Fluids PediatricДокумент2 страницыPaeds IV Fluids PediatricotakmesumОценок пока нет
- Vol-2 Issue-1 Approach To Respiratory Distress in The Newborn 19Документ13 страницVol-2 Issue-1 Approach To Respiratory Distress in The Newborn 19salamredОценок пока нет
- By Nur Fatin Najihah Binti NoruddinДокумент7 страницBy Nur Fatin Najihah Binti NoruddinNajihah NoruddinОценок пока нет
- What Is ForexДокумент8 страницWhat Is ForexnurzuriatyОценок пока нет
- Case Digest Labor DisputeДокумент5 страницCase Digest Labor DisputeMysh PDОценок пока нет
- ENVSOCTY 1HA3 - Lecture 01 - Introduction & Course Overview - Skeletal NotesДокумент28 страницENVSOCTY 1HA3 - Lecture 01 - Introduction & Course Overview - Skeletal NotesluxsunОценок пока нет
- Cap 1 Intro To Business Communication Format NouДокумент17 страницCap 1 Intro To Business Communication Format NouValy ValiОценок пока нет
- Finlatics Investment Banking Experience ProgramДокумент4 страницыFinlatics Investment Banking Experience ProgramSameer BheriОценок пока нет
- Icmap Newsletter June 2017Документ7 страницIcmap Newsletter June 2017GoopОценок пока нет
- Settling The Debate On Birth Order and PersonalityДокумент2 страницыSettling The Debate On Birth Order and PersonalityAimanОценок пока нет
- Projectile Motion PhysicsДокумент3 страницыProjectile Motion Physicsapi-325274340Оценок пока нет
- Possessive Adjectives 3Документ1 страницаPossessive Adjectives 3RAMIRO GARCIA CANCELAОценок пока нет
- The American New CriticsДокумент5 страницThe American New CriticsSattigul KharakozhaОценок пока нет
- ) Mark Scheme (Results) January 2019: Pearson Edexcel International GCSE in Mathematics A (4MA1) Higher Tier Paper 1HRДокумент22 страницы) Mark Scheme (Results) January 2019: Pearson Edexcel International GCSE in Mathematics A (4MA1) Higher Tier Paper 1HRNewtonОценок пока нет
- Allusions and References - 5Документ3 страницыAllusions and References - 5Matthew HallingОценок пока нет
- The Christ of NankingДокумент7 страницThe Christ of NankingCarlos PérezОценок пока нет
- Business Information Systems 2021: Cardiff Metropolitan UniversityДокумент30 страницBusiness Information Systems 2021: Cardiff Metropolitan UniversityMichelle FernandoОценок пока нет
- Introducing Identity - SummaryДокумент4 страницыIntroducing Identity - SummarylkuasОценок пока нет
- GrandEsta - Double Eyelid Surgery PDFДокумент2 страницыGrandEsta - Double Eyelid Surgery PDFaniyaОценок пока нет
- Mactor Report - Taller de Prospectiva D 2Документ39 страницMactor Report - Taller de Prospectiva D 2Giovani Alexis Saez VegaОценок пока нет
- Guoyin Shen, Ho-Kwang Mao and Russell J. Hemley - Laser-Heated Diamond Anvil Cell Technique: Double-Sided Heating With Multimode Nd:YAG LaserДокумент5 страницGuoyin Shen, Ho-Kwang Mao and Russell J. Hemley - Laser-Heated Diamond Anvil Cell Technique: Double-Sided Heating With Multimode Nd:YAG LaserDeez34PОценок пока нет
- Novel Synthesis of BarbituratesДокумент3 страницыNovel Synthesis of BarbituratesRafaella Ferreira100% (2)
- Chapter 1 (Research)Документ6 страницChapter 1 (Research)Salome CarpioОценок пока нет
- Agreement - AFS - RERA Punjab 20190906pro - Forma - Agreement - of - Sale - To - Be - Signed - With - AllotteesДокумент35 страницAgreement - AFS - RERA Punjab 20190906pro - Forma - Agreement - of - Sale - To - Be - Signed - With - AllotteesPuran Singh LabanaОценок пока нет
- Practice Test 12 Use of English I. Choose The Best AnswerДокумент6 страницPractice Test 12 Use of English I. Choose The Best AnswerJack NguyễnОценок пока нет