Вам также может понравиться
- Objective - Subjective Eye Examination-Referral System and When To ReferДокумент56 страницObjective - Subjective Eye Examination-Referral System and When To ReferClara Sainuka100% (1)
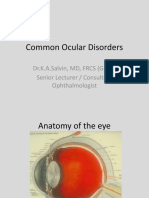
- Common Ocular DisordersДокумент108 страницCommon Ocular DisordersKa SalvinОценок пока нет
- Sree Teja-OphthalmologyДокумент56 страницSree Teja-OphthalmologysanjuОценок пока нет
- Examination Technique of The Eye & Ophthalmic EquipmentsДокумент59 страницExamination Technique of The Eye & Ophthalmic Equipmentshenok birukОценок пока нет
- Sensation: Hearing, Vision, Taste, Touch, and SmellДокумент99 страницSensation: Hearing, Vision, Taste, Touch, and SmellMichelle LindsayОценок пока нет
- AcquiredCataractДокумент30 страницAcquiredCataractYouhengОценок пока нет
- Cataract SenilisДокумент54 страницыCataract Senilismayo djitroОценок пока нет
- Gradual Loss of Vision-Nurses - 065937Документ73 страницыGradual Loss of Vision-Nurses - 065937CosbyОценок пока нет
- HYPERMETROPIA and Myopia PDFДокумент55 страницHYPERMETROPIA and Myopia PDFDrashti ChudasamaОценок пока нет
- Glaucoma & CataractДокумент53 страницыGlaucoma & CataractBenita100% (1)
- AMETROPIAДокумент48 страницAMETROPIARahul KirkОценок пока нет
- Cataract Qustion and AnswersДокумент90 страницCataract Qustion and AnswersVaishnavi MОценок пока нет
- L6 Refractive Errors and PaedsДокумент37 страницL6 Refractive Errors and PaedsSofíaGriggsОценок пока нет
- Mishermaliyani I11105026Документ49 страницMishermaliyani I11105026Dewi rafikaОценок пока нет
- Cataract 3Документ11 страницCataract 3Ravi KushwahaОценок пока нет
- Cataract: Done by Jony MallikДокумент46 страницCataract: Done by Jony MallikAlfa Suryani ArdliОценок пока нет
- Cataract: Done by Mo3taz Abu Rabiah A7mad LubaniДокумент46 страницCataract: Done by Mo3taz Abu Rabiah A7mad LubaniMaxwell C Jay KafwaniОценок пока нет
- Cataract 1 Lecture PmcajkДокумент33 страницыCataract 1 Lecture PmcajkAbdul Munim KhanОценок пока нет
- Cataract 1 MBBS Lecture by Prof Munim SuriДокумент33 страницыCataract 1 MBBS Lecture by Prof Munim SuriMunim SuriОценок пока нет
- Opthalmic Emergencies PresentationДокумент85 страницOpthalmic Emergencies PresentationvictoreffiomОценок пока нет
- Cataracts: ClassificationДокумент9 страницCataracts: ClassificationRafay ChacharОценок пока нет
- Refractive ErrorsДокумент33 страницыRefractive ErrorsMathew Sebastian100% (2)
- Degenerative MyopiaДокумент53 страницыDegenerative MyopiaNiloy BasakОценок пока нет
- Vision Impairment 1Документ59 страницVision Impairment 1122ritik goyalОценок пока нет
- Case Report ODS Immature Senile Cataract: Devi Indah Permatasari 111 2016 2137Документ43 страницыCase Report ODS Immature Senile Cataract: Devi Indah Permatasari 111 2016 2137SuardimanAchoОценок пока нет
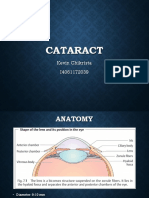
- Cataract: Kevin Chikrista I4061172039Документ18 страницCataract: Kevin Chikrista I4061172039Kevin ChikristaОценок пока нет
- Geraitric Examination of EyeДокумент37 страницGeraitric Examination of Eyetanishqa eye careОценок пока нет
- LensДокумент46 страницLensDr Sravya M VОценок пока нет
- 1 CataractДокумент31 страница1 CataractsnehalОценок пока нет
- Loss of Vision IДокумент61 страницаLoss of Vision IMUBIRU SAMUEL EDWARDОценок пока нет
- DR Ajai Agrawal Additional Professor Department of Ophthalmology AIIMS RishikeshДокумент48 страницDR Ajai Agrawal Additional Professor Department of Ophthalmology AIIMS RishikeshSrishti KhullarОценок пока нет
- LECTURE 8 Vitreous - Peripheral Retina PathologyДокумент60 страницLECTURE 8 Vitreous - Peripheral Retina PathologyOknitaLasmainiОценок пока нет
- Impaired Vision and BlindnessДокумент44 страницыImpaired Vision and BlindnessYujenОценок пока нет
- 7 Lens and Cataract 1Документ57 страниц7 Lens and Cataract 1Devi Melissa RiupassaОценок пока нет
- Trauma To The GlobeДокумент19 страницTrauma To The Globejollyday90Оценок пока нет
- RefraksiДокумент84 страницыRefraksinaroetocapkutilОценок пока нет
- Common Eye Diseases 2022Документ33 страницыCommon Eye Diseases 2022Shia LevyОценок пока нет
- Examination of EyeДокумент39 страницExamination of EyeDr Sravya M VОценок пока нет
- Phacoantigenic Response To Ruptured Lens Capsule: Clinicopathologic CaseДокумент20 страницPhacoantigenic Response To Ruptured Lens Capsule: Clinicopathologic Casefm_askaОценок пока нет
- Cataract: BY: Huda Hamdan Rubaalsheyab Maramalanbar AbeerhussainДокумент59 страницCataract: BY: Huda Hamdan Rubaalsheyab Maramalanbar AbeerhussainaliОценок пока нет
- Congenital CataractДокумент27 страницCongenital CataractbharatpurhosОценок пока нет
- UNIVERSITY OF MEDICAL SCIENCES"REZONANCA"-Halil Ajvazi/Ophthalmology/Prishtina/Republic of KosovaДокумент98 страницUNIVERSITY OF MEDICAL SCIENCES"REZONANCA"-Halil Ajvazi/Ophthalmology/Prishtina/Republic of KosovaHALIL Z.AJVAZI100% (1)
- Chapter 11 Eye & Vision DisordersДокумент72 страницыChapter 11 Eye & Vision DisordersMYLENE GRACE ELARCOSAОценок пока нет
- Ocular ExaminationДокумент49 страницOcular Examinationkushraj khandelwalОценок пока нет
- Materi KatarakДокумент39 страницMateri KatarakfebyОценок пока нет
- Congenital CataractsДокумент123 страницыCongenital CataractsRizqy AbdullahОценок пока нет
- Ophthalmology EmergenciesДокумент60 страницOphthalmology Emergenciesasraf amirullahОценок пока нет
- Ophthalmology Clerks: Alea, Denz Marc Custodio, Audreyfil Perez, Francis MiguelДокумент14 страницOphthalmology Clerks: Alea, Denz Marc Custodio, Audreyfil Perez, Francis MiguelDenz Marc AleaОценок пока нет
- MyopiaДокумент9 страницMyopiaNavani TharanОценок пока нет
- OT 677 Conditions Lecture 3Документ66 страницOT 677 Conditions Lecture 3Yuvaraaj NavaneethakrishnanОценок пока нет
- Eye Disorders: Structure of The EyeДокумент13 страницEye Disorders: Structure of The Eyeapi-3822433Оценок пока нет
- CATARACTДокумент12 страницCATARACTTaiwo IfedolapoОценок пока нет
- Painful Dimn of VisionДокумент19 страницPainful Dimn of VisionVidushi AgarwalОценок пока нет
- Opt Halm OlogyДокумент87 страницOpt Halm OlogyAya MahmoudОценок пока нет
- GLAUKOMAДокумент47 страницGLAUKOMARahma GhnОценок пока нет
- Concomitant Squint: Noor Asmah MD Azmi Optometrist HsahДокумент56 страницConcomitant Squint: Noor Asmah MD Azmi Optometrist HsahAnonymous l2Fve4PpD33% (3)
- Anisman Acute Vision LossДокумент68 страницAnisman Acute Vision Lossarnol3090Оценок пока нет
- Congenital Glaucoma FinalДокумент48 страницCongenital Glaucoma FinalMona MohammedОценок пока нет
- Low Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsОт EverandLow Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsОценок пока нет
- Visual Field Loss in the Real World: A Book of Static Perimetry Test Targets for Eye Health ProfessionalsОт EverandVisual Field Loss in the Real World: A Book of Static Perimetry Test Targets for Eye Health ProfessionalsОценок пока нет
- Case Based Ophthalmology GuideДокумент12 страницCase Based Ophthalmology GuideGradestack100% (2)
- Optical Instrument: By: Sariyati, S.TДокумент21 страницаOptical Instrument: By: Sariyati, S.TparamitaОценок пока нет
- Color History TerminologyДокумент21 страницаColor History TerminologysefiefОценок пока нет
- Lesson Plan in Science and HealthДокумент3 страницыLesson Plan in Science and HealthKennan Azor100% (1)
- Psych c61 Midterm2 ReviewДокумент26 страницPsych c61 Midterm2 ReviewKate SongОценок пока нет
- Prevention of Hyperopic SurpriseДокумент4 страницыPrevention of Hyperopic SurpriseDavid MartínezОценок пока нет
- SensorialДокумент6 страницSensorialPatrick DaniardОценок пока нет
- Physiology of HearingДокумент45 страницPhysiology of HearingJP SouaidОценок пока нет
- Ophthalmologists in BC 2011 DecДокумент14 страницOphthalmologists in BC 2011 Decbaby_goatОценок пока нет
- Optic Nerve: Applied AnatomyДокумент10 страницOptic Nerve: Applied AnatomyMariam QaisОценок пока нет
- Ophtalmology Record Acute Glaucoma: Examiner: DR. Dr. Gilbert W. Simanjuntak, SP.M (K)Документ6 страницOphtalmology Record Acute Glaucoma: Examiner: DR. Dr. Gilbert W. Simanjuntak, SP.M (K)Rashellya RasyidaОценок пока нет
- CRANIAL Nerves - ExaminationДокумент14 страницCRANIAL Nerves - ExaminationMoussa FarhatОценок пока нет
- Waisbourd 2019Документ9 страницWaisbourd 2019Leandro LopezОценок пока нет
- Functional Vision Assessment Standard 8Документ5 страницFunctional Vision Assessment Standard 8api-315690330Оценок пока нет
- Electro Physiology of VisionДокумент528 страницElectro Physiology of VisionYazmin Peñaloza RoaОценок пока нет
- GR 3 Science 1st 4thДокумент335 страницGR 3 Science 1st 4thKrey100% (1)
- Sensory System - PathwaysДокумент25 страницSensory System - PathwaysHamid Hussain HamidОценок пока нет
- Contact Lenses Fitting GuideДокумент40 страницContact Lenses Fitting Guidemoni7777Оценок пока нет
- PY40 - BIO - GROUP3The Somatic Nervous SystemДокумент22 страницыPY40 - BIO - GROUP3The Somatic Nervous SystemAdéọlá OnasanyaОценок пока нет
- Visually Guided Eye Movements Reduce Postural Sway in Dyslexic ChildrenДокумент6 страницVisually Guided Eye Movements Reduce Postural Sway in Dyslexic ChildrenGabriella FigueiredoОценок пока нет
- Muhammad Irfan: Pendidikan SkillsДокумент1 страницаMuhammad Irfan: Pendidikan SkillsmataiwakОценок пока нет
- Kwame Nkrumah University of Science and Technology: College of Health Sciences School of Medical SciencesДокумент25 страницKwame Nkrumah University of Science and Technology: College of Health Sciences School of Medical SciencesEmmanuel DanquahОценок пока нет
- ProP - Differentiating Nuclear Sclerosis From CataractsДокумент6 страницProP - Differentiating Nuclear Sclerosis From CataractsDita TaepangОценок пока нет
- AphakiaДокумент12 страницAphakiaankur_1Оценок пока нет
- Sony XBR-55HX929 CNET Review Calibration ResultsДокумент7 страницSony XBR-55HX929 CNET Review Calibration ResultsDavid KatzmaierОценок пока нет
- Visual Perceptual Dysfunctions and Assessment: Made By:gundeep Singh MOT NeurologyДокумент74 страницыVisual Perceptual Dysfunctions and Assessment: Made By:gundeep Singh MOT NeurologyPaloma McОценок пока нет
- Understanding ColorДокумент24 страницыUnderstanding Colorroludju roludjuОценок пока нет
- Cros and Bicros Devices: Minimum Hearing Loss Threshold (MHLT) CriteriaДокумент1 страницаCros and Bicros Devices: Minimum Hearing Loss Threshold (MHLT) CriteriaFahmil AgungОценок пока нет
- Black Vestibular DisordersДокумент102 страницыBlack Vestibular DisorderskimОценок пока нет
- Chapter 47 Sensory ReceptorsДокумент3 страницыChapter 47 Sensory ReceptorsrehassanОценок пока нет