Вам также может понравиться
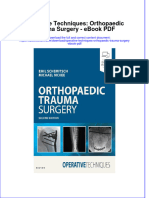
- Abdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019Документ46 страницAbdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019AmmarОценок пока нет
- HerniaДокумент8 страницHerniaعبد المعطي الجماعيОценок пока нет
- The Abdominal WallДокумент32 страницыThe Abdominal WallarshmeentariqОценок пока нет
- Hernia IngunalisДокумент29 страницHernia Ingunalisyaodoe1Оценок пока нет
- Inguinal and Femoral HerniaДокумент50 страницInguinal and Femoral HerniaFafa NabihaОценок пока нет
- Medscape Abdominal HerniasДокумент47 страницMedscape Abdominal HerniasSary OktiviaОценок пока нет
- Hernias: Dr. Kosov E.V., Department of Surgery and OSTAДокумент53 страницыHernias: Dr. Kosov E.V., Department of Surgery and OSTAprashant singhОценок пока нет
- Hernia: Done by D1 GroupДокумент47 страницHernia: Done by D1 Groupanindyadputri100% (1)
- Hernias (Inguinal and Femoral)Документ37 страницHernias (Inguinal and Femoral)Muwanga faizoОценок пока нет
- Hernias: General Features To All Types of HerniasДокумент19 страницHernias: General Features To All Types of Herniashussain AltaherОценок пока нет
- Umbilical HerniaДокумент1 страницаUmbilical HerniaShameer Mohamed AljabarОценок пока нет
- GS2 HerniaДокумент13 страницGS2 HerniaMAH pedОценок пока нет
- Hernia - Femoral Hernia, Epigastric Hernia, Paraumbilical Hernia, Incisional HerniaДокумент29 страницHernia - Femoral Hernia, Epigastric Hernia, Paraumbilical Hernia, Incisional HerniaKuruОценок пока нет
- Abdominal Wall HerniasДокумент29 страницAbdominal Wall Herniasbunny_totsОценок пока нет
- HerniaДокумент47 страницHerniamalathiОценок пока нет
- HerniaДокумент46 страницHerniaZubairkhan SuraniОценок пока нет
- Inguinal Hernias: CaseДокумент6 страницInguinal Hernias: Casechomz14Оценок пока нет
- Submitted By:: Balacang, Karen L. N-416 Group A Cluster 2 Mr. Raymund P. Bautista RN MAN Clinical Instructor at TCHДокумент26 страницSubmitted By:: Balacang, Karen L. N-416 Group A Cluster 2 Mr. Raymund P. Bautista RN MAN Clinical Instructor at TCHKim BalacangОценок пока нет
- Deviriligo Notes 12Документ99 страницDeviriligo Notes 12A Fish100% (1)
- Types of Hernia and Its ManagementДокумент80 страницTypes of Hernia and Its ManagementVisaagan Kalaithasan50% (2)
- Hernia1 InguinalДокумент7 страницHernia1 InguinalmunafalmahdiОценок пока нет
- AbdWall, Hernia Atbp - AnnoДокумент34 страницыAbdWall, Hernia Atbp - AnnoJuan Lorenzo RequironОценок пока нет
- Hernias MBCHB LectureДокумент31 страницаHernias MBCHB LectureAb BabyОценок пока нет
- Hernia AbdominalisДокумент45 страницHernia AbdominalisFAIRUZ RIFANIОценок пока нет
- Impression HerniaДокумент3 страницыImpression Herniakjeseo8Оценок пока нет
- Lo 5Документ13 страницLo 5Mutiara Prima DianaОценок пока нет
- HerniaДокумент100 страницHerniaangelaanapaku100% (3)
- Eventrații Și EviscerațiiДокумент55 страницEventrații Și EviscerațiiPanuta AndrianОценок пока нет
- Hernia Seminar 2 Aug 2014 FinalДокумент20 страницHernia Seminar 2 Aug 2014 FinalKishan NaiduОценок пока нет
- Abdominal Wall HerniaДокумент100 страницAbdominal Wall Herniaintandiahningrum100% (1)
- 2019 Hernia Kuliah FKДокумент50 страниц2019 Hernia Kuliah FKKhairani NurhamidahОценок пока нет
- General Consideration Inguinal Hernias: Femoral Hernia Incisional Hernia Umbilial Hernia Hernia of Linea AlbaДокумент30 страницGeneral Consideration Inguinal Hernias: Femoral Hernia Incisional Hernia Umbilial Hernia Hernia of Linea Albainna3003Оценок пока нет
- Classification & Investigations of HerniaДокумент56 страницClassification & Investigations of HerniaFobin VargheseОценок пока нет
- Diseses of Large IntestineДокумент24 страницыDiseses of Large Intestineaastharawat1234Оценок пока нет
- Abdominal Hernia: Jama Patient PageДокумент1 страницаAbdominal Hernia: Jama Patient PageSherly CanceritaОценок пока нет
- HerniaДокумент67 страницHerniaياسر نعيم الربيعي100% (1)
- Abdominal Wall HerniasДокумент14 страницAbdominal Wall HerniasDarawan MirzaОценок пока нет
- Hernia: DR - Surender Singh DhankharДокумент36 страницHernia: DR - Surender Singh DhankharBharat BhushanОценок пока нет
- HerniaДокумент106 страницHerniaDr-Mohammad Ali-Fayiz Al TamimiОценок пока нет
- Abdominal Wall, Omentum, Mesentery and Retroperitoneum DR AsepkyДокумент33 страницыAbdominal Wall, Omentum, Mesentery and Retroperitoneum DR Asepkyafwan fajriОценок пока нет
- HerniaДокумент34 страницыHerniaSisay FentaОценок пока нет
- Hernia: DR - Kaushik Patel, MPT Assistant Professor SPB Physiotherapy CollegeДокумент43 страницыHernia: DR - Kaushik Patel, MPT Assistant Professor SPB Physiotherapy CollegeSalman KhanОценок пока нет
- Anatomy BLOCK II Clinical CorrelatesДокумент15 страницAnatomy BLOCK II Clinical CorrelatesAshley BuchananОценок пока нет
- What Is Hernia?: Hernia Occurs When An Organ or Fatty TissueДокумент47 страницWhat Is Hernia?: Hernia Occurs When An Organ or Fatty TissuePhuntsho OngmoОценок пока нет
- HerniaДокумент79 страницHernianorhafizahstoh89Оценок пока нет
- Hernias: Daniel IgoДокумент46 страницHernias: Daniel Igobigboss80s100% (1)
- Key PointsДокумент34 страницыKey PointsSe YunОценок пока нет
- HerniaДокумент12 страницHerniaAdelia Maharani DОценок пока нет
- Inguinal HerniaДокумент37 страницInguinal HerniaAb Baby100% (1)
- Hernia Scrotalis FIxДокумент56 страницHernia Scrotalis FIxivaniОценок пока нет
- HerniaДокумент34 страницыHerniaUmair FirdousОценок пока нет
- Femoral HerniaДокумент3 страницыFemoral HerniakhurshidghorihumaОценок пока нет
- Injuries To The Birth CanalДокумент67 страницInjuries To The Birth CanalnamitaОценок пока нет
- HERNIAДокумент3 страницыHERNIAisaacpapicaОценок пока нет
- CASE PRESENTATION Nadhirah RahimДокумент60 страницCASE PRESENTATION Nadhirah RahimNadhirah Rahim100% (1)
- Hernia, (Different Types) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHernia, (Different Types) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsРейтинг: 5 из 5 звезд5/5 (1)
- Pleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsОт EverandPleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsОценок пока нет
- Graston TechniqueДокумент8 страницGraston TechniqueSvetlana PolyakovaОценок пока нет
- Goddess DurgaДокумент6 страницGoddess DurgaanjalibhatsОценок пока нет
- A Case of Homicidal Bride Burning: An Analysis of Variables: Chaitanya Mittal, Suraj SundaragiriДокумент3 страницыA Case of Homicidal Bride Burning: An Analysis of Variables: Chaitanya Mittal, Suraj SundaragiriTri YulihartiОценок пока нет
- Exercises For IT Band SyndromeДокумент3 страницыExercises For IT Band Syndromeamirreza jmОценок пока нет
- WOD - Mage - The Ascension - The Horizon War Trilogy Book 3 - War in Heaven PDFДокумент378 страницWOD - Mage - The Ascension - The Horizon War Trilogy Book 3 - War in Heaven PDFShanito Not'onbut'off67% (3)
- SpondyloarthritisДокумент77 страницSpondyloarthritisRapid MedicineОценок пока нет
- PARM LBP CPG 2nd Edition 2017 PDFДокумент293 страницыPARM LBP CPG 2nd Edition 2017 PDFGumDropОценок пока нет
- Wire Rope Application - HandbookДокумент64 страницыWire Rope Application - HandbookhhanehОценок пока нет
- Physical AssessmentДокумент19 страницPhysical Assessmentsilentscream0618Оценок пока нет
- Emergency Care in NursingДокумент32 страницыEmergency Care in NursingPauline Añes100% (1)
- Neuroanatomy TractsДокумент7 страницNeuroanatomy TractsLola PОценок пока нет
- Psoas StretchesДокумент9 страницPsoas Stretcheswalterego58Оценок пока нет
- For Information For Review For Approval For Construction As-BuiltДокумент21 страницаFor Information For Review For Approval For Construction As-BuiltUtku Can KılıçОценок пока нет
- Genito Urinary TraumaДокумент16 страницGenito Urinary TraumaAjibola OlamideОценок пока нет
- 10 003591 01EN FlexoFORM User PDFДокумент86 страниц10 003591 01EN FlexoFORM User PDFSabino LaraОценок пока нет
- Ebook Operative Techniques Orthopaedic Trauma Surgery PDF Full Chapter PDFДокумент67 страницEbook Operative Techniques Orthopaedic Trauma Surgery PDF Full Chapter PDFcynthia.mcclendon928100% (22)
- Navara D40Документ352 страницыNavara D40Hard ManОценок пока нет
- Dawson 2002 - Upper-Extremity Problems Caused by Playing InstrumentsДокумент6 страницDawson 2002 - Upper-Extremity Problems Caused by Playing InstrumentsDiana MatiasОценок пока нет
- Field Density Testing GuideДокумент32 страницыField Density Testing Guidenikita6969Оценок пока нет
- Joint Trauma System Clinical Practice Guideline (Jts CPG)Документ30 страницJoint Trauma System Clinical Practice Guideline (Jts CPG)nnnn hhhhОценок пока нет
- Forensic ScienceДокумент19 страницForensic ScienceParamjit SinghОценок пока нет
- Wheeless' Textbook of OrthopaedicsДокумент6 страницWheeless' Textbook of Orthopaedicsnurul auliaОценок пока нет
- Mes 3Документ4 страницыMes 3Johnpeter EsporlasОценок пока нет
- Bedside Radiography Othopedic Implats Lecture R. LAVADIAДокумент34 страницыBedside Radiography Othopedic Implats Lecture R. LAVADIADreu GlennОценок пока нет
- Pawanmuktasana - Part IIДокумент21 страницаPawanmuktasana - Part IIHazel100% (3)
- 915 Mini-Zoom: Service ManualДокумент42 страницы915 Mini-Zoom: Service ManualccarltonОценок пока нет
- 6th Body Systems Packet WORKSHEETSДокумент39 страниц6th Body Systems Packet WORKSHEETSElizabeth Alvarez100% (1)
- Anatomy Notes 1:28:2019Документ4 страницыAnatomy Notes 1:28:2019Taylor IgnarriОценок пока нет
- Zimmer Natural Nail System Cephalomedullary Standard Nail Surgical TechniqueДокумент40 страницZimmer Natural Nail System Cephalomedullary Standard Nail Surgical Techniqueasdar fajrinОценок пока нет
- General Safety - It's Your DecisionДокумент1 страницаGeneral Safety - It's Your Decisionserdar yücelОценок пока нет