Вам также может понравиться
- GVHDДокумент35 страницGVHDSaad KhanОценок пока нет
- HIV Notes (Clinical Virology) MR - ManigaДокумент31 страницаHIV Notes (Clinical Virology) MR - ManigaDaniel OkakaОценок пока нет
- DR - Dr.efrida Warganegara, M.Kes., SP - MKДокумент30 страницDR - Dr.efrida Warganegara, M.Kes., SP - MKDedy SantosoОценок пока нет
- HIV Life Cycle: Scott M. Hammer, M.DДокумент7 страницHIV Life Cycle: Scott M. Hammer, M.DMohammad SalemyОценок пока нет
- Biology Ip XiiДокумент8 страницBiology Ip XiiSugumaran MageshОценок пока нет
- Nursing Clients With HIV Infection and AIDS: Learning ObjectivesДокумент11 страницNursing Clients With HIV Infection and AIDS: Learning Objectivesmorynayim-1Оценок пока нет
- Nri1201 Hiv PosterДокумент1 страницаNri1201 Hiv Posteranirbanmanna88320100% (1)
- Hepatitis CCRN KFSH&RC Asma AlshehriДокумент33 страницыHepatitis CCRN KFSH&RC Asma AlshehriasmashОценок пока нет
- Acquired Immuno-Deficiency Syndrome (AIDS) : Savitha R S JSSCP, MysoreДокумент41 страницаAcquired Immuno-Deficiency Syndrome (AIDS) : Savitha R S JSSCP, MysorerathanОценок пока нет
- Is HivДокумент50 страницIs HivRodriguez, Jhe-ann M.Оценок пока нет
- CD Hiv-Aids PDF ReviewerДокумент33 страницыCD Hiv-Aids PDF ReviewerMeryville JacildoОценок пока нет
- Session 6 L Blood Borne Viruses HIV HVДокумент62 страницыSession 6 L Blood Borne Viruses HIV HVBlendma AhmedОценок пока нет
- Lec 6Документ32 страницыLec 6Ghadi AbdalazizОценок пока нет
- Acquired Immunodeficiency Syndrome (AIDS) : Faridha S IlyasДокумент73 страницыAcquired Immunodeficiency Syndrome (AIDS) : Faridha S IlyasElearning FK UnhasОценок пока нет
- Virology-2 MergedДокумент258 страницVirology-2 MergedLogyn SamОценок пока нет
- HivДокумент29 страницHivSUTHAN100% (2)
- Pertemuan Ke-2 REPROДокумент74 страницыPertemuan Ke-2 REPROAdi Joyo NegoroОценок пока нет
- Presented By:-Pallavi Chawla Pallavi Dhiman (BDS - 3 Year)Документ28 страницPresented By:-Pallavi Chawla Pallavi Dhiman (BDS - 3 Year)tinu989Оценок пока нет
- HIV - AIDS and Immunocompromised (With Notes)Документ94 страницыHIV - AIDS and Immunocompromised (With Notes)Ali YousefОценок пока нет
- HIV InfectionДокумент47 страницHIV InfectionMarwanОценок пока нет
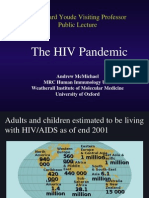
- The HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureДокумент50 страницThe HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureSanthosh SubramanianОценок пока нет
- AIDSДокумент32 страницыAIDSJuwairia tariqОценок пока нет
- Human Immuno Deficiency Virus (Hiv) : By: Muluneh T. (MSC in Medical Microbiology)Документ65 страницHuman Immuno Deficiency Virus (Hiv) : By: Muluneh T. (MSC in Medical Microbiology)Tilahun TesemaОценок пока нет
- Antibiogram Perdalin FeraIbrahimДокумент62 страницыAntibiogram Perdalin FeraIbrahimTJANG RICKY CHANDRAОценок пока нет
- Human Immunodeficency VirusДокумент58 страницHuman Immunodeficency VirusRandy BerryОценок пока нет
- HIV&HepatitisДокумент100 страницHIV&HepatitisRaja RuzannaОценок пока нет
- HIV Infection / AIDS (Z21, B20-B24)Документ37 страницHIV Infection / AIDS (Z21, B20-B24)Shreya ThackerОценок пока нет
- Pertemuan Ke-2 REPROДокумент74 страницыPertemuan Ke-2 REPROMohamad Rheza F ZamzamiОценок пока нет
- (Human Immunodeficiency Virus) &: Acquired Immune Deficiency SyndromeДокумент61 страница(Human Immunodeficiency Virus) &: Acquired Immune Deficiency SyndromeGufron MustofaОценок пока нет
- Case Study PPT - PDF HIV With Opportunistic Infection - Madayag March 2023Документ71 страницаCase Study PPT - PDF HIV With Opportunistic Infection - Madayag March 2023Rasheda PickettОценок пока нет
- Diagnostic Fungal Antigens 23032023 ME BougnouxVF 110035Документ86 страницDiagnostic Fungal Antigens 23032023 ME BougnouxVF 110035Sabi MaalemОценок пока нет
- Human Immunodeficiency Virus (HIV) : Mohammad Al-Rawashdeh 54-5th CourseДокумент39 страницHuman Immunodeficiency Virus (HIV) : Mohammad Al-Rawashdeh 54-5th CourseMohammadSAL-RawashdehОценок пока нет
- DengueДокумент44 страницыDengueAl JihadОценок пока нет
- Hiv and AidsДокумент23 страницыHiv and Aidsjigyansh25Оценок пока нет
- Manifestasi Klinis HIVДокумент111 страницManifestasi Klinis HIVFebrina EvaОценок пока нет
- Aids and Immunodeficiencies: - Kiruthika ManivannanДокумент35 страницAids and Immunodeficiencies: - Kiruthika ManivannanrevaishОценок пока нет
- Delfin, RMTДокумент34 страницыDelfin, RMTAffie SaikolОценок пока нет
- 3 Pulmonary Fungal and Viral Infections Part 3 Viruses and UnusualДокумент28 страниц3 Pulmonary Fungal and Viral Infections Part 3 Viruses and UnusualjimmyneumologiaОценок пока нет
- Viral Infections in Humans Basics: Dr.T.V.Rao MDДокумент94 страницыViral Infections in Humans Basics: Dr.T.V.Rao MDariffdrОценок пока нет
- Post Op InfectionsДокумент62 страницыPost Op InfectionsDr.Rudra PrasadОценок пока нет
- UNIT 4 - New Challenges: Urja JoshiДокумент72 страницыUNIT 4 - New Challenges: Urja JoshiRadhey RavalОценок пока нет
- RetrovirusesДокумент79 страницRetrovirusesrasimmozturkОценок пока нет
- VirusДокумент57 страницVirusSophan HadieОценок пока нет
- AIDS Teaching ModuleДокумент122 страницыAIDS Teaching Moduletummalapalli venkateswara raoОценок пока нет
- Dynamics of Disease TransmissionДокумент30 страницDynamics of Disease TransmissionSyed Sanan shahОценок пока нет
- Hiv / Aids Education & Prevention ProgramДокумент36 страницHiv / Aids Education & Prevention ProgramselvianaОценок пока нет
- Hiv Seminar 2019Документ49 страницHiv Seminar 2019clarice_condeno100% (1)
- Presented By: Marlene Lombi C T SiviaДокумент19 страницPresented By: Marlene Lombi C T SiviaVanlal RemruatiОценок пока нет
- Overview of HIV and Its Management: Caroline Mills-Davies Emmanuel FantevieДокумент101 страницаOverview of HIV and Its Management: Caroline Mills-Davies Emmanuel FantevieImanuel Fantevie100% (1)
- The Person Living With: Hiv/Disease Hiv/DiseaseДокумент59 страницThe Person Living With: Hiv/Disease Hiv/DiseasejaydipОценок пока нет
- Dr. Ridho - HIVДокумент20 страницDr. Ridho - HIVpenizubaediОценок пока нет
- Immunodeficiency: Abdul Ghaffar, Ph.D. E-Mail: Ghaffar@med - Sc.eduДокумент10 страницImmunodeficiency: Abdul Ghaffar, Ph.D. E-Mail: Ghaffar@med - Sc.eduAhmed Goma'aОценок пока нет
- Transfusion Transmitted InfectionsДокумент30 страницTransfusion Transmitted InfectionsSadio KeitaОценок пока нет
- Hepatitis Viruses ÍõÅà ÕДокумент85 страницHepatitis Viruses ÍõÅà Õrasool ghaffariОценок пока нет
- HIV Replicação e PatogeneseДокумент33 страницыHIV Replicação e Patogenesejose ribamar borges mendesОценок пока нет
- Human Immunodeficiency Virus (Hiv)Документ50 страницHuman Immunodeficiency Virus (Hiv)kiran kcОценок пока нет
- Immunology 8Документ37 страницImmunology 8ukashazam19Оценок пока нет
- Pertemuan Ke-2 REPROДокумент74 страницыPertemuan Ke-2 REPROAbi Surya MandalaОценок пока нет
- Aesthetic Facial Anatomy Essentials For Injections-CRC Press (2020)Документ259 страницAesthetic Facial Anatomy Essentials For Injections-CRC Press (2020)stella95% (22)
- 1 of 1 - My Health SummaryДокумент210 страниц1 of 1 - My Health SummaryCandace DeihlОценок пока нет
- Case-Digest-Imbong-V-Ochoa Part 2Документ6 страницCase-Digest-Imbong-V-Ochoa Part 2Kate Hazzle JandaОценок пока нет
- DIASS Quarter1 Module 1Документ24 страницыDIASS Quarter1 Module 1JoshОценок пока нет
- Bio-Data of Foreigen Domestic Worker (FDW)Документ6 страницBio-Data of Foreigen Domestic Worker (FDW)azriannaОценок пока нет
- Professional Teacher Secondary (Science) 03-2024Документ20 страницProfessional Teacher Secondary (Science) 03-2024PRC BaguioОценок пока нет
- Week 4 DiscussionДокумент1 страницаWeek 4 DiscussionJacob YorgОценок пока нет
- Sex Usually Comes To Mind When We Hear The WordsДокумент1 страницаSex Usually Comes To Mind When We Hear The WordsCheryl PetersenОценок пока нет
- Nursing Leadership and Management Practice TestДокумент1 страницаNursing Leadership and Management Practice TestMikhaela GonzalesОценок пока нет
- MENTOR 13 Lionel Rammamurthy Oet For NursingДокумент4 страницыMENTOR 13 Lionel Rammamurthy Oet For NursingAnjana Varghese0% (1)
- Undergrad ThesisДокумент42 страницыUndergrad ThesisJoe Bryant LaguerderОценок пока нет
- SHPS Health Care Reimbursement Claim FormДокумент3 страницыSHPS Health Care Reimbursement Claim FormmlbissОценок пока нет
- LAVOISIER RINGER LACTATE, Solution For InfusionДокумент2 страницыLAVOISIER RINGER LACTATE, Solution For InfusionNaia RenitaОценок пока нет
- Brazilian Journal of Physical TherapyДокумент12 страницBrazilian Journal of Physical TherapyKen ABОценок пока нет
- Employment Reference Letter - Cognizant Technology SolutionДокумент3 страницыEmployment Reference Letter - Cognizant Technology Solutionshaikh Tabrez AlamОценок пока нет
- Patient SafetyДокумент25 страницPatient Safetyfbasudan2Оценок пока нет
- Encyclopedia of Survey Research Methods - Lavrakas - 2008 PDFДокумент1 041 страницаEncyclopedia of Survey Research Methods - Lavrakas - 2008 PDFhelton_bsb84% (25)
- PNS 293 National Food Control SystemДокумент24 страницыPNS 293 National Food Control SystemSherry SalazarОценок пока нет
- Fbao Protocols Conscious To Unconscious - Infant Care (2010 Ecc Guidelines Applied)Документ1 страницаFbao Protocols Conscious To Unconscious - Infant Care (2010 Ecc Guidelines Applied)Aleksandar PetrovicОценок пока нет
- Changing Our Understanding of HealthДокумент4 страницыChanging Our Understanding of HealthYuliana DewiОценок пока нет
- Managing Time For Success in CollegeДокумент2 страницыManaging Time For Success in CollegeKeziah SantosОценок пока нет
- Body at Home by Jorge Cruise - ExcerptДокумент44 страницыBody at Home by Jorge Cruise - ExcerptCrown Publishing Group86% (35)
- Oak Tree Union Colored Cemetery of TaylorvilleДокумент14 страницOak Tree Union Colored Cemetery of TaylorvilleWFTVОценок пока нет
- (PHARMACEUTICS-II, 2131) : Diploma in Pharmacy 2Nd Year: E-Learning ContentДокумент2 страницы(PHARMACEUTICS-II, 2131) : Diploma in Pharmacy 2Nd Year: E-Learning Contentkamlesh singhОценок пока нет
- Ginny An Analysis of Knowledge Attitude and Practices Regarding Standard Precautions of Infection Control and Impact of Knowledge and Attitude of ICU Nurses On Self-Reported Practices of InfДокумент7 страницGinny An Analysis of Knowledge Attitude and Practices Regarding Standard Precautions of Infection Control and Impact of Knowledge and Attitude of ICU Nurses On Self-Reported Practices of InfMANISHA FMSОценок пока нет
- Case Simulation 3 in Pediatric NursingДокумент3 страницыCase Simulation 3 in Pediatric NursingCaren MarquezОценок пока нет
- 4.method Statement - Installation of FRP Lining For Steel Tank Rev02Документ4 страницы4.method Statement - Installation of FRP Lining For Steel Tank Rev02Sripathi SeetharamanОценок пока нет
- Infection Control NurseДокумент41 страницаInfection Control NurseChris-Goldie Lorezo100% (1)
- Magic CardДокумент2 страницыMagic CardbedabyashmirdhaОценок пока нет
- Rhu Nutrition ProgramДокумент12 страницRhu Nutrition ProgrampapayОценок пока нет