Вам также может понравиться
- Pharmacoeconomics: Presented By: M. Krishna Aishwarya M. Pharmacy Ii/Ii Year Drug Regulatory AffairsДокумент16 страницPharmacoeconomics: Presented By: M. Krishna Aishwarya M. Pharmacy Ii/Ii Year Drug Regulatory AffairsaishuОценок пока нет
- PhaaaaДокумент101 страницаPhaaaaWesam MazenОценок пока нет
- Clinical Pharmacology: Proceedings of the 7th International Congress of Pharmacology, Paris 1978От EverandClinical Pharmacology: Proceedings of the 7th International Congress of Pharmacology, Paris 1978P. Duchêne-MarullazОценок пока нет
- Methods of Pharmacoeconomic AnalysisДокумент19 страницMethods of Pharmacoeconomic AnalysisDoaa BadarnehОценок пока нет
- Counselling, Concordance, and Communication - Innovative Education For PharmacistsДокумент50 страницCounselling, Concordance, and Communication - Innovative Education For PharmacistsSurampalliGuruОценок пока нет
- Lecture 1. Introduction To Clinical PharmacyДокумент14 страницLecture 1. Introduction To Clinical Pharmacydaniya nadeem100% (1)
- 1 - Pharmaceutical Care Practice - An OverviewДокумент76 страниц1 - Pharmaceutical Care Practice - An OverviewekramОценок пока нет
- Exam 2 AДокумент6 страницExam 2 Aapi-3723612Оценок пока нет
- PharmacoeconomicsДокумент54 страницыPharmacoeconomicsAsfa MarediaОценок пока нет
- Journal Club Template: For Randomized Controlled TrialsДокумент19 страницJournal Club Template: For Randomized Controlled TrialsAndrew DavidsonОценок пока нет
- Types of Economic and Humanistic Outcomes AssessmentsДокумент47 страницTypes of Economic and Humanistic Outcomes AssessmentsPharmacotherapyОценок пока нет
- Immunization Policy Guidline - Kenya 2013Документ72 страницыImmunization Policy Guidline - Kenya 2013okwadha simionОценок пока нет
- Adherence and Medication Adherence Rating Scale (MARS)Документ4 страницыAdherence and Medication Adherence Rating Scale (MARS)International Journal of Innovative Science and Research TechnologyОценок пока нет
- Application of PK in Clinical SitutionДокумент42 страницыApplication of PK in Clinical Situtionsafia mehmood100% (1)
- Pharmacists Role Clinical Pharmacokinetic MonitoringДокумент2 страницыPharmacists Role Clinical Pharmacokinetic MonitoringauliaОценок пока нет
- Two-Compartment Extravascular ModelДокумент16 страницTwo-Compartment Extravascular ModelNeha Gulfam100% (1)
- Section 1 Quiz (Due July 5th) - PHAR 1001 (001) Orientation To Pharmacy (Summer 2019)Документ13 страницSection 1 Quiz (Due July 5th) - PHAR 1001 (001) Orientation To Pharmacy (Summer 2019)Shu YeeОценок пока нет
- Biopharmacy Full Text PDFДокумент173 страницыBiopharmacy Full Text PDFEimy NaomyОценок пока нет
- Polypharmacy PDFДокумент9 страницPolypharmacy PDFsheryl maeОценок пока нет
- A Textbook of Clinical Pharmacy PracticeДокумент6 страницA Textbook of Clinical Pharmacy PracticeOdyОценок пока нет
- Drug InteractionsДокумент5 страницDrug Interactionsvajkember100% (1)
- Therapeutics Handbook 2014 - 140804 PDFДокумент384 страницыTherapeutics Handbook 2014 - 140804 PDFEnvhy WinaОценок пока нет
- Contraceptive Pharmacology Katz Com 2010Документ41 страницаContraceptive Pharmacology Katz Com 2010Michael KatzОценок пока нет
- Amity Institute of Pharmacy-NddsДокумент5 страницAmity Institute of Pharmacy-NddsTanujaОценок пока нет
- Bio Availability and Bio EquivalenceДокумент32 страницыBio Availability and Bio Equivalenceكسلان اكتب اسمي100% (1)
- Health Economics&PharmacoeconomicsДокумент89 страницHealth Economics&PharmacoeconomicsRasvini RajendranОценок пока нет
- Factors Affecting Drug Metabolism PDFДокумент2 страницыFactors Affecting Drug Metabolism PDFPaige50% (2)
- IPPE 1 Community Workbook Class of 2020Документ65 страницIPPE 1 Community Workbook Class of 2020Anonymous hF5zAdvwCCОценок пока нет
- TDM of LidocaineДокумент19 страницTDM of LidocaineNikkiiОценок пока нет
- Ward RoundДокумент2 страницыWard RoundAnonymous whcvnPBeQОценок пока нет
- Pharmaceutical CareДокумент27 страницPharmaceutical Caremai elewaОценок пока нет
- Type 2 DM: New Onset: Patient PresentationДокумент3 страницыType 2 DM: New Onset: Patient PresentationShailu Gracie BalacuitОценок пока нет
- B. Informatics (Slides 1-66)Документ7 страницB. Informatics (Slides 1-66)Chrissy LayugОценок пока нет
- Incompatibility IV AdmixtureДокумент17 страницIncompatibility IV AdmixtureClara Herlina100% (1)
- Pharmacoeconomic Analysis WorksheetДокумент3 страницыPharmacoeconomic Analysis WorksheetCatalina Dumitru100% (1)
- Pharmaceutical Calculations PHT 210Документ34 страницыPharmaceutical Calculations PHT 210Fitri Nurussani AuliaОценок пока нет
- Internationalinformationpack 2011Документ20 страницInternationalinformationpack 2011manzurqadirОценок пока нет
- Communication Skills in Pharmacy Practice: Dr. Hiwak. SaaedДокумент70 страницCommunication Skills in Pharmacy Practice: Dr. Hiwak. SaaedAnonymous whcvnPBeQОценок пока нет
- Pharmacy PracticeДокумент17 страницPharmacy PracticeP D SpencerОценок пока нет
- Ethics in Pharmacy Practice 200910 PDFДокумент38 страницEthics in Pharmacy Practice 200910 PDFjohnassesОценок пока нет
- Statement of Principle Self-Care Including Self-Medication - The Professional Role of The PharmacistДокумент5 страницStatement of Principle Self-Care Including Self-Medication - The Professional Role of The PharmacistAprilia R. Permatasari0% (1)
- Chapter 5 Ethics in Pharmacy PracticeДокумент13 страницChapter 5 Ethics in Pharmacy PracticeKhairi Mustafa Salem100% (1)
- Causality Assessment PharmacovigilanceДокумент8 страницCausality Assessment PharmacovigilanceAnonymous Q0wdNI9Оценок пока нет
- Labelling and PackagingДокумент16 страницLabelling and PackagingvyshnosudhaОценок пока нет
- Introduction To BiopharmaceuticsДокумент27 страницIntroduction To BiopharmaceuticsAmina Akther Mim 1821179649Оценок пока нет
- General Prescribing Guidelines of Pedriatic PatientsДокумент11 страницGeneral Prescribing Guidelines of Pedriatic PatientsGloomi100% (1)
- 4 Fields of Practice of PharmacyДокумент28 страниц4 Fields of Practice of PharmacyEmmanuel Lomocso Pinsoy Jr.Оценок пока нет
- Essential of PharmacoeconomicsДокумент313 страницEssential of PharmacoeconomicsDevika Munisamy100% (3)
- Def of Forensic Pharmacy by FatimaДокумент7 страницDef of Forensic Pharmacy by FatimaTofeeque Ali GhouriОценок пока нет
- Comunity Pharmacy Introduction ModДокумент42 страницыComunity Pharmacy Introduction ModPrity girlОценок пока нет
- Mathematical Fundamental in PharmacokineticДокумент21 страницаMathematical Fundamental in PharmacokineticErna PratiwiОценок пока нет
- Altered Pharmacokinetics in Liver DiseasesДокумент30 страницAltered Pharmacokinetics in Liver DiseasesNailaAns100% (1)
- Brex CVS DrugsДокумент287 страницBrex CVS DrugsKate EvangelistaОценок пока нет
- Pharmacy: Undergraduate Study 2016Документ18 страницPharmacy: Undergraduate Study 2016kgiyerОценок пока нет
- Pharmacotherapy of HTNДокумент57 страницPharmacotherapy of HTNAbera JamboОценок пока нет
- Profesi Unjani Dispensing TechniquesДокумент26 страницProfesi Unjani Dispensing TechniquesNur AjiОценок пока нет
- Preventing Dispensing ErrorsДокумент39 страницPreventing Dispensing ErrorsMark RevertОценок пока нет
- The Role of The Pharmacist in The Health Care SystemДокумент6 страницThe Role of The Pharmacist in The Health Care SystemZain AlviОценок пока нет
- 7-Renal Function TestsДокумент4 страницы7-Renal Function TestsAhmed ImranОценок пока нет
- Betnovate C For Acne Scars: 6 Betamethasone Valerate Foam PriceДокумент7 страницBetnovate C For Acne Scars: 6 Betamethasone Valerate Foam PriceAhmed ImranОценок пока нет
- 6-Liver Function TestsДокумент5 страниц6-Liver Function TestsAhmed ImranОценок пока нет
- Clinical Portal Hyoer TensionДокумент8 страницClinical Portal Hyoer TensionAhmed ImranОценок пока нет
- Drug Interactions - Case StudiesДокумент2 страницыDrug Interactions - Case StudiesAhmed Imran75% (4)
- Peptic Ulcer Clinical PharmacyДокумент4 страницыPeptic Ulcer Clinical PharmacyAhmed ImranОценок пока нет
- Galenical PreperationДокумент35 страницGalenical PreperationAhmed ImranОценок пока нет
- Non-Aqueous TitrationsДокумент40 страницNon-Aqueous TitrationsAhmed Imran100% (2)
- 6-Liver Function TestsДокумент5 страниц6-Liver Function TestsAhmed ImranОценок пока нет
- Toxins and ToxoidsДокумент18 страницToxins and ToxoidsAhmed ImranОценок пока нет
- Clinical Use of Herbs & Herbal Medicine inДокумент17 страницClinical Use of Herbs & Herbal Medicine inAhmed ImranОценок пока нет
- ReactionДокумент54 страницыReactionAhmed ImranОценок пока нет
- Antifungalgel PDFДокумент18 страницAntifungalgel PDFAhmed ImranОценок пока нет
- Rhe OlogyДокумент48 страницRhe OlogyAhmed ImranОценок пока нет
- Muhammad Wajid: Institute of Pharmacy Gulab Devi Educational Complex, LahoreДокумент31 страницаMuhammad Wajid: Institute of Pharmacy Gulab Devi Educational Complex, LahoreAhmed ImranОценок пока нет
- Topical Tinctures: Submitted byДокумент17 страницTopical Tinctures: Submitted byAhmed Imran100% (1)
- MCQ - Pharmacology LippincottДокумент48 страницMCQ - Pharmacology Lippincottamwritea82% (22)
- Pharm.D, M.phil Lecturer PharmacognosyДокумент32 страницыPharm.D, M.phil Lecturer PharmacognosyAhmed ImranОценок пока нет
- Plant HormonesДокумент40 страницPlant HormonesAhmed ImranОценок пока нет
- Antidiuretic Hormone: Muhammad Wajid Assistant ProfessorДокумент20 страницAntidiuretic Hormone: Muhammad Wajid Assistant ProfessorAhmed ImranОценок пока нет
- Extracts and Fluid ExtractsДокумент14 страницExtracts and Fluid ExtractsAhmed ImranОценок пока нет
- All FormulaДокумент4 страницыAll FormulaAhmed ImranОценок пока нет
- Miscellaneous ProcessesДокумент103 страницыMiscellaneous ProcessesAhmed Imran75% (4)
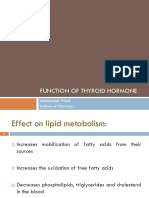
- Function of Thyroid Hormone: Muhammad Wajid Institute of PharmacyДокумент14 страницFunction of Thyroid Hormone: Muhammad Wajid Institute of PharmacyAhmed ImranОценок пока нет
- 000536454-Guidebook To Mechanism in Organic Chemistry PDFДокумент214 страниц000536454-Guidebook To Mechanism in Organic Chemistry PDFJennifer Carolina Rosales NoriegaОценок пока нет
- Allergy: Pharm .D, M. Phil Lecturer (Pharmacognosy)Документ35 страницAllergy: Pharm .D, M. Phil Lecturer (Pharmacognosy)Ahmed Imran0% (1)
- Allosteric EnzymeДокумент22 страницыAllosteric EnzymeAhmed ImranОценок пока нет
- Biosynthesis of Fatty Acids-1Документ25 страницBiosynthesis of Fatty Acids-1Ahmed ImranОценок пока нет
- Allosteric EnzymeДокумент22 страницыAllosteric EnzymeAhmed Imran100% (1)
- Cebu City Medical Center-College of NursingДокумент5 страницCebu City Medical Center-College of NursingJimnah Rhodrick BontilaoОценок пока нет
- Intermittent Fasting Vs Daily Calorie Restriction For Type 2 Diabetes Prevention: A Review of Human FindingsДокумент10 страницIntermittent Fasting Vs Daily Calorie Restriction For Type 2 Diabetes Prevention: A Review of Human FindingsAmry Irsyada YusufОценок пока нет
- Lisa Parks - Meghan Routt - Oncology Nursing Society Staff - Critical Care Nursing of The Oncology Patient-Oncology Nursing Society (2018)Документ512 страницLisa Parks - Meghan Routt - Oncology Nursing Society Staff - Critical Care Nursing of The Oncology Patient-Oncology Nursing Society (2018)Bejusca ToniОценок пока нет
- The Complete CBT Guide For Depression and Low MoodДокумент642 страницыThe Complete CBT Guide For Depression and Low Moodalanbray115Оценок пока нет
- Supervivencia Dental A Largo Plazo Después Del Tratamiento Regenerativo de Defectos IntraóseosДокумент7 страницSupervivencia Dental A Largo Plazo Después Del Tratamiento Regenerativo de Defectos IntraóseosAgustin BuryakОценок пока нет
- Neonatal JaundiceДокумент7 страницNeonatal JaundiceAnas ObiedОценок пока нет
- Surgical Sponges - Towels WebДокумент20 страницSurgical Sponges - Towels WebDa Josh MarienellaОценок пока нет
- Complicaciones Mini ImplantesДокумент12 страницComplicaciones Mini ImplantesNuvia PardoОценок пока нет
- Antimicrobial Stewardship Program (Ri)Документ50 страницAntimicrobial Stewardship Program (Ri)Erni Yessyca SimamoraОценок пока нет
- Beliefs of Filipino Caregivers On Occupational Therapy Through TelehealthДокумент4 страницыBeliefs of Filipino Caregivers On Occupational Therapy Through TelehealthBETINA NICOLE SYОценок пока нет
- Chronic DiseaseДокумент13 страницChronic DiseaseDanielle MadeОценок пока нет
- W 26882Документ53 страницыW 26882Jose GueraОценок пока нет
- Csir Life Sciences Fresh Instant NotesДокумент4 страницыCsir Life Sciences Fresh Instant NotesAlps Ana33% (3)
- 2014 Group Case StudyДокумент42 страницы2014 Group Case StudyBrian100% (1)
- Osce History Taking Evaluation Form 2022Документ1 страницаOsce History Taking Evaluation Form 2022Jill SunОценок пока нет
- Diet and Its TypesДокумент11 страницDiet and Its Typesanita100% (1)
- Ocupol D Drops and Ointment PDFДокумент3 страницыOcupol D Drops and Ointment PDFAnushka ShresthaОценок пока нет
- Clear Vacancy R2Документ696 страницClear Vacancy R2bhuviОценок пока нет
- 1078-Texto Del Artículo-2743-1-10-20171030 PDFДокумент12 страниц1078-Texto Del Artículo-2743-1-10-20171030 PDFRichard Copa AliОценок пока нет
- Ayurveda at KaivalyadhamaДокумент8 страницAyurveda at KaivalyadhamaAnshumaan SinghОценок пока нет
- Stock Opname 2022Документ9 страницStock Opname 2022laboratorium rsitОценок пока нет
- Health StatisticsДокумент43 страницыHealth Statisticsramanand chaudharyОценок пока нет
- Appropriate Maximum Phlebotomy Volumes: Neonate, Infant and Pediatric PopulationДокумент2 страницыAppropriate Maximum Phlebotomy Volumes: Neonate, Infant and Pediatric PopulationEthiopia HagereОценок пока нет
- Tiered Response AgreementДокумент3 страницыTiered Response AgreementThe Hamilton SpectatorОценок пока нет
- HypertensionДокумент22 страницыHypertensionLubeeha HaselОценок пока нет
- Role of Nurse Hospitalized ChildДокумент29 страницRole of Nurse Hospitalized ChildAjay Remya100% (2)
- Manchester Anaemia GuideДокумент13 страницManchester Anaemia Guidemubzy14Оценок пока нет
- Antihypertensive Drugs - Classification and SynthesisДокумент14 страницAntihypertensive Drugs - Classification and SynthesisCường NguyễnОценок пока нет
- INDIVIDUAL Assignment For The Course Inclusiveness (SNIE 1012) (15%) For Engineering S and Applied A, B, & C Groups Instruction I: Choose The Best Answer For The Ten Questions That FollowДокумент3 страницыINDIVIDUAL Assignment For The Course Inclusiveness (SNIE 1012) (15%) For Engineering S and Applied A, B, & C Groups Instruction I: Choose The Best Answer For The Ten Questions That FollowErmi ZuruОценок пока нет
- Ensuring Patient Comfort and Clinical Accuracy During Impression Taking 3Документ11 страницEnsuring Patient Comfort and Clinical Accuracy During Impression Taking 3Raul HernandezОценок пока нет