Вам также может понравиться
- SUPERHERO Suspension Training ManualДокумент11 страницSUPERHERO Suspension Training ManualCaleb Leadingham100% (5)
- Pre-Op Preparation and Assessment of Pediatric PatientsДокумент62 страницыPre-Op Preparation and Assessment of Pediatric PatientsBedahanakugmОценок пока нет
- Readers Digest November 2021 PDF RD 2021 PDF EnglishДокумент172 страницыReaders Digest November 2021 PDF RD 2021 PDF EnglishIslam Gold100% (1)
- Krisis Tiroid FixДокумент38 страницKrisis Tiroid FixVita DesriantiОценок пока нет
- 3rd Nutrimet 2019 PROCEEDING BOOK PDFДокумент82 страницы3rd Nutrimet 2019 PROCEEDING BOOK PDFPutri NasutionОценок пока нет
- Week 3Документ396 страницWeek 3Danica Mae BianitoОценок пока нет
- Corn Fact Book 2010Документ28 страницCorn Fact Book 2010National Corn Growers AssociationОценок пока нет
- Capacitor BanksДокумент49 страницCapacitor BanksAmal P RaviОценок пока нет
- Hamed2016Документ4 страницыHamed2016Franknanda D'enzieroX-zhirawaxaveriuz PutrascreamoDark-nataseОценок пока нет
- Management Terapi Cairan Dr. AW 01Документ60 страницManagement Terapi Cairan Dr. AW 01Umhy GumianaОценок пока нет
- Penyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUДокумент56 страницPenyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUFitriana WijayatiОценок пока нет
- Kegawatdaruratan Pada Anak Dan Bayi: Kepaniteraan Klinik Emergensi RSUP Fatmawati Jakarta FKIK UIN Syarif HidayatullahДокумент81 страницаKegawatdaruratan Pada Anak Dan Bayi: Kepaniteraan Klinik Emergensi RSUP Fatmawati Jakarta FKIK UIN Syarif HidayatullahJavar SodicОценок пока нет
- Fluid TherapyДокумент56 страницFluid TherapyHabibie El RamadhaniОценок пока нет
- Acute Coronary Syndrome 052014Документ91 страницаAcute Coronary Syndrome 052014Fatahillah NazarОценок пока нет
- Ventilasi Mekanik Untuk Neonatus: Dr. R. Adhi Teguh Perma Iskandar Sp.A Divisi Perinatologi FKUI-RSCMДокумент52 страницыVentilasi Mekanik Untuk Neonatus: Dr. R. Adhi Teguh Perma Iskandar Sp.A Divisi Perinatologi FKUI-RSCMireneaureliaОценок пока нет
- Pediatri Essensial 3Документ86 страницPediatri Essensial 3Gregorius WahyudiОценок пока нет
- PowderCoatingResins ProductGuide 0Документ20 страницPowderCoatingResins ProductGuide 0zizitroОценок пока нет
- PertusisДокумент28 страницPertusiswenyinriantoОценок пока нет
- SepsisДокумент16 страницSepsisDaniela100% (1)
- Akut AbdomenДокумент24 страницыAkut AbdomenSelingkuhan neptunusОценок пока нет
- Gagal Napas: Pembimbing Dr. Ngakan Putu Parsama Putra, SPP (K) Presenter Dr. Muli YamanДокумент20 страницGagal Napas: Pembimbing Dr. Ngakan Putu Parsama Putra, SPP (K) Presenter Dr. Muli YamanAdlan BinharyantoОценок пока нет
- Terapi Cairan: Pembimbing: Dr. Dr. Bobby Setiadi Dharmawan, SpaДокумент45 страницTerapi Cairan: Pembimbing: Dr. Dr. Bobby Setiadi Dharmawan, SpaAdamilzaryFikryОценок пока нет
- Management Terapi CairanДокумент60 страницManagement Terapi Cairanpeter singalОценок пока нет
- PAT + Primary SurveyДокумент33 страницыPAT + Primary Surveysalsa100% (1)
- Fluid ResponsivenessДокумент70 страницFluid Responsivenessrina febriatiОценок пока нет
- Dr. dadang-RESUSITASI DERESUSITASI CAIRAN ANAK SAKITKkRITIS DADANG - KONIKA17 JOGJA 11 Agustus 17 - OK PDFДокумент52 страницыDr. dadang-RESUSITASI DERESUSITASI CAIRAN ANAK SAKITKkRITIS DADANG - KONIKA17 JOGJA 11 Agustus 17 - OK PDFBetty HijrahОценок пока нет
- Ilmu Kesehatan Anak: Judul Materi: Pendekatan Anemia Pada AnakДокумент103 страницыIlmu Kesehatan Anak: Judul Materi: Pendekatan Anemia Pada AnakDhanin WitedjaОценок пока нет
- Fluid Managementuntuk Mahasiswa SajaДокумент56 страницFluid Managementuntuk Mahasiswa SajaPratami Rieuwpassa IIОценок пока нет
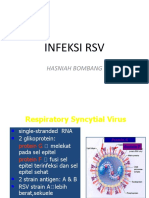
- Infeksi RSV: Hasniah BombangДокумент12 страницInfeksi RSV: Hasniah Bombangmuh hardiansyahОценок пока нет
- IPDIДокумент30 страницIPDIaris budionoОценок пока нет
- Anaesthesia SummaryДокумент36 страницAnaesthesia SummaryRazan QassemОценок пока нет
- PPDS - AR - 22 16 - Agu - P Ilovepdf Compressed Ilovepdf C PDFДокумент192 страницыPPDS - AR - 22 16 - Agu - P Ilovepdf Compressed Ilovepdf C PDFlaboratorium rshmdn100% (1)
- Monitoring OF Hemorrhagic Shock: Basrul HanafiДокумент24 страницыMonitoring OF Hemorrhagic Shock: Basrul HanafiabdurrahmanОценок пока нет
- Lapsus Dr. DodyДокумент36 страницLapsus Dr. DodyPriscilla Christina NatanОценок пока нет
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Документ17 страницKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaОценок пока нет
- Diabetic FootДокумент73 страницыDiabetic Footmohammad.irfanОценок пока нет
- FCPS Pulmonogy CPSP Course BookletДокумент32 страницыFCPS Pulmonogy CPSP Course BookletQiblaHazoor100% (1)
- Print Recognition and Assessment of The Seriously Ill Patient - Dr. SupartoДокумент20 страницPrint Recognition and Assessment of The Seriously Ill Patient - Dr. SupartoSianipar Mangara Wahyu CharrosОценок пока нет
- MalariaДокумент23 страницыMalariaIBhe Damianry QritezzОценок пока нет
- Children With Henoch Schonlein Purpura 2.0Документ13 страницChildren With Henoch Schonlein Purpura 2.0soniaОценок пока нет
- Kuliah Pengayaan DM 2017-1Документ100 страницKuliah Pengayaan DM 2017-1Syarifah Maharani HidayatОценок пока нет
- What Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)Документ39 страницWhat Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)laurentiaОценок пока нет
- Japanese EncephalitisДокумент14 страницJapanese EncephalitisMuhammad Rafli AkbarОценок пока нет
- Tatalaksana Awal Koreksi Cairan Pada Kasus Syok - Dr. Rudy K, SP - PDДокумент60 страницTatalaksana Awal Koreksi Cairan Pada Kasus Syok - Dr. Rudy K, SP - PDmuhammad benyОценок пока нет
- Bunga Rampai Infeksi Dengue AnakДокумент67 страницBunga Rampai Infeksi Dengue AnakSatrio PrimaesoОценок пока нет
- 1-Fluid Management in Critically Ill Patients - Update Int Med Feb2018Документ46 страниц1-Fluid Management in Critically Ill Patients - Update Int Med Feb2018ดนุ เกษรศิริОценок пока нет
- Mengenal Resusitasi Pada Anak Dan Bayi Bagi Perawat PemulaДокумент15 страницMengenal Resusitasi Pada Anak Dan Bayi Bagi Perawat PemulaSiti Krisan WijayaОценок пока нет
- Mengenal Kegawatan Pada AnakДокумент45 страницMengenal Kegawatan Pada Anakyasmin100% (1)
- Neonatal CholestasisДокумент5 страницNeonatal CholestasisMateen ShukriОценок пока нет
- MVDBWP VP ZL UP3 L 4 V5 XH G1636761573Документ23 страницыMVDBWP VP ZL UP3 L 4 V5 XH G1636761573Ummu muzhaffarОценок пока нет
- Rational Blood Transfusion in Infant and ChildrenДокумент37 страницRational Blood Transfusion in Infant and ChildrenBayu KurniawanОценок пока нет
- Guidelines 2015 Ed3Документ318 страницGuidelines 2015 Ed3MonicaLadyMelohОценок пока нет
- Resusitasi NeonatusДокумент22 страницыResusitasi NeonatusnikkitaihsanОценок пока нет
- Clabsi DR - RonaldДокумент19 страницClabsi DR - RonaldsilviОценок пока нет
- Pediatric: Abdulrahman Y. SabbaghДокумент36 страницPediatric: Abdulrahman Y. SabbaghAbdulrahman Y. SabbaghОценок пока нет
- Cme Acs 2. Stemi (Izzah)Документ36 страницCme Acs 2. Stemi (Izzah)Hakimah K. SuhaimiОценок пока нет
- Stunting (EDIT)Документ62 страницыStunting (EDIT)846035Оценок пока нет
- K21-Fever With RashДокумент76 страницK21-Fever With RashMarisa Perucana SinambelaОценок пока нет
- Surviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedДокумент32 страницыSurviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedAdli Wafi Jabbar100% (1)
- 2 DHF InternaДокумент59 страниц2 DHF Internasaladass 2Оценок пока нет
- Malaria Management Asep MCU FinalДокумент65 страницMalaria Management Asep MCU FinalTommy JunaidiОценок пока нет
- Body Fluids: Dr. Deepthi de Silva Senior Lecturer Department of PhysiologyДокумент34 страницыBody Fluids: Dr. Deepthi de Silva Senior Lecturer Department of PhysiologyRukshan RanatungaОценок пока нет
- Fluid ManagementДокумент10 страницFluid ManagementdradaadОценок пока нет
- Fluid and Electrolyte ReplacementДокумент60 страницFluid and Electrolyte ReplacementAlex WagnerОценок пока нет
- Fluid Management & Shock ResuscitationДокумент35 страницFluid Management & Shock ResuscitationAmel MelatiОценок пока нет
- RB Boiler Product SpecsДокумент4 страницыRB Boiler Product Specsachmad_silmiОценок пока нет
- Gmail - RedBus Ticket - TN7R20093672Документ2 страницыGmail - RedBus Ticket - TN7R20093672Bappa RoyОценок пока нет
- Narrative ReporДокумент3 страницыNarrative ReporMARK LUKE ULITОценок пока нет
- CPhI Japan InformationДокумент22 страницыCPhI Japan InformationctyvteОценок пока нет
- Grounds of Divorce Under Hindu Religion or Hindu Law Unit-A: Chapter-IiДокумент42 страницыGrounds of Divorce Under Hindu Religion or Hindu Law Unit-A: Chapter-IiSatyam PathakОценок пока нет
- HumareaderДокумент37 страницHumareaderStefan JovanovicОценок пока нет
- Preservation and Collection of Biological EvidenceДокумент4 страницыPreservation and Collection of Biological EvidenceanastasiaОценок пока нет
- Course Syllabus Manufacturing Processes (1) Metal CuttingДокумент4 страницыCourse Syllabus Manufacturing Processes (1) Metal CuttingG. Dancer GhОценок пока нет
- Pengaruh Penambahan Lateks Pada Campuran Asphalt Concrete Binder Course (AC-BC)Документ10 страницPengaruh Penambahan Lateks Pada Campuran Asphalt Concrete Binder Course (AC-BC)Haris FirdausОценок пока нет
- Recommendation On The Acquisation of VitasoyДокумент8 страницRecommendation On The Acquisation of Vitasoyapi-237162505Оценок пока нет
- Seven-Year Financial Pro Jection: ProblemДокумент10 страницSeven-Year Financial Pro Jection: Problemnyashadzashe munyatiОценок пока нет
- Understanding Senior Citizens Outlook of Death Sample FormatДокумент14 страницUnderstanding Senior Citizens Outlook of Death Sample FormatThea QuibuyenОценок пока нет
- Laws and Regulation Related To FoodДокумент33 страницыLaws and Regulation Related To FoodDr. Satish JangraОценок пока нет
- Capacity Requirement PlanningДокумент17 страницCapacity Requirement PlanningvamsibuОценок пока нет
- Hydrogen Production From The Air: Nature CommunicationsДокумент9 страницHydrogen Production From The Air: Nature CommunicationsdfdffОценок пока нет
- Rar Vol11 Nro3Документ21 страницаRar Vol11 Nro3Valentine WijayaОценок пока нет
- Astm A712 PDFДокумент3 страницыAstm A712 PDFCristian OtivoОценок пока нет
- SRV SLB222 en - 05062020Документ2 страницыSRV SLB222 en - 05062020Nguyen ThuongОценок пока нет
- Moderated Caucus Speech Samples For MUNДокумент2 страницыModerated Caucus Speech Samples For MUNihabОценок пока нет
- Compensation ManagementДокумент2 страницыCompensation Managementshreekumar_scdlОценок пока нет
- FINALE Final Chapter1 PhoebeKatesMDelicanaPR-IIeditedphoebe 1Документ67 страницFINALE Final Chapter1 PhoebeKatesMDelicanaPR-IIeditedphoebe 1Jane ParkОценок пока нет
- Calculation Condensation StudentДокумент7 страницCalculation Condensation StudentHans PeterОценок пока нет
- PSB 3441 CH 1 HallucinogensДокумент2 страницыPSB 3441 CH 1 HallucinogensAnonymous lm3GIU45Оценок пока нет
- Module 2: Environmental Science: EcosystemДокумент8 страницModule 2: Environmental Science: EcosystemHanna Dia MalateОценок пока нет
- Deloitte Uk Mining and Metals DecarbonizationДокумент10 страницDeloitte Uk Mining and Metals DecarbonizationfpreuscheОценок пока нет