Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- KPJ Healthcare University College: Bph1073 Dosage Form Design and Dispensing IiДокумент4 страницыKPJ Healthcare University College: Bph1073 Dosage Form Design and Dispensing IiamrhkmhОценок пока нет
- Eng1103 Group WorkДокумент3 страницыEng1103 Group WorkamrhkmhОценок пока нет
- Argumentative Essay Revision NotesДокумент3 страницыArgumentative Essay Revision NotesamrhkmhОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Transitionwordsargue PDFДокумент2 страницыTransitionwordsargue PDFamrhkmhОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- English Script PresentationДокумент9 страницEnglish Script PresentationamrhkmhОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Thesis Statement Intro and ConclusionДокумент2 страницыThesis Statement Intro and ConclusionamrhkmhОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Suppositories and Pessaries - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008)Документ7 страницSuppositories and Pessaries - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008)amrhkmhОценок пока нет
- Activity 2-Semi Solid Products - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008)Документ8 страницActivity 2-Semi Solid Products - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008)amrhkmhОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Suppositories and Pessaries - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008)Документ7 страницSuppositories and Pessaries - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008)amrhkmhОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- SUPPOSITORIES CBL - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008) BPH7Документ4 страницыSUPPOSITORIES CBL - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008) BPH7amrhkmh100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Marketed Oral Powders - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008)Документ7 страницMarketed Oral Powders - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008)amrhkmhОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Surat Iringan Bi KMJДокумент1 страницаSurat Iringan Bi KMJamrhkmhОценок пока нет
- Activity 1 - Semi Solid Products - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008 (Документ12 страницActivity 1 - Semi Solid Products - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008 (amrhkmhОценок пока нет
- Ointment - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008)Документ8 страницOintment - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008)amrhkmhОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Summary of Reaction Pathways in Organic ChemistryДокумент4 страницыSummary of Reaction Pathways in Organic ChemistryMohd Rais Faiq NicholОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Experiment #8: Aldehydes and KetonesДокумент12 страницExperiment #8: Aldehydes and Ketonesamrhkmh100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- CBL Assignment Organic ChemistryДокумент11 страницCBL Assignment Organic ChemistryamrhkmhОценок пока нет
- Substitution Reactions (S 2 Versus S 1) : Chemistry 5.12 Spring 2003, Handout #9Документ2 страницыSubstitution Reactions (S 2 Versus S 1) : Chemistry 5.12 Spring 2003, Handout #9amrhkmhОценок пока нет
- EliminationДокумент18 страницEliminationIshaan ChaturvediОценок пока нет
- Elimination ReactionsДокумент19 страницElimination ReactionsanantОценок пока нет
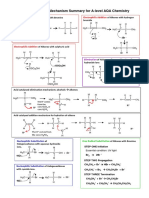
- Mechanism Summary For A-Level AQA Chemistry: BR BRДокумент5 страницMechanism Summary For A-Level AQA Chemistry: BR BRamrhkmhОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Surat Sokongan Bi KMJДокумент1 страницаSurat Sokongan Bi KMJamrhkmhОценок пока нет
- 14 sn12 Highlights PDFДокумент6 страниц14 sn12 Highlights PDFSonali SarkarОценок пока нет
- Stereochemistry PDFДокумент6 страницStereochemistry PDFamrhkmhОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Ulasan Artikel - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008) PDFДокумент5 страницUlasan Artikel - Siti Amirah Hakimah Binti Mohd Fairuz (2062191008) PDFamrhkmhОценок пока нет
- Exercise Ready To PSPM, Matriculation (Science Computer)Документ7 страницExercise Ready To PSPM, Matriculation (Science Computer)amrhkmh100% (1)
- ROAD TO PROGRAMmingДокумент2 страницыROAD TO PROGRAMmingamrhkmhОценок пока нет
- Tutorial 1-ANSДокумент7 страницTutorial 1-ANSamrhkmhОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- ENG 1103 English For Healthcare ProfessionalsДокумент2 страницыENG 1103 English For Healthcare ProfessionalsamrhkmhОценок пока нет
- Branham - Transfusion Medicine Instructional PlanДокумент12 страницBranham - Transfusion Medicine Instructional Planapi-610404410Оценок пока нет
- Post Test MS RleДокумент15 страницPost Test MS RleAngel YN Patricio FlorentinoОценок пока нет
- CAP Transfusion Medicine Checklist 2013Документ86 страницCAP Transfusion Medicine Checklist 2013oliut74Оценок пока нет
- Manual of Standards For Blood Collection Units in The PhilippinesДокумент89 страницManual of Standards For Blood Collection Units in The PhilippinesBlue PielagoОценок пока нет
- Ponciano IH PDFДокумент69 страницPonciano IH PDFCaressa Marie EstradaОценок пока нет
- Private Health Institutions LawДокумент22 страницыPrivate Health Institutions LawShankar Sanyal100% (1)
- Dr. Mohammed H Saiemaldahr Blood Bank Med Tech Dep @kaauДокумент20 страницDr. Mohammed H Saiemaldahr Blood Bank Med Tech Dep @kaauKristiann lourine ProvidoОценок пока нет
- Biopure CorporationДокумент23 страницыBiopure CorporationKabir RoshannОценок пока нет
- Gap Report Astha HospitalДокумент49 страницGap Report Astha HospitalNidhi VijanОценок пока нет
- Minimum Requirements For Blood Bank Compliance With Article 14 Traceability and Article 15 Notification of Serious Adverse Reactions and Events of EU Directive 200298ECДокумент37 страницMinimum Requirements For Blood Bank Compliance With Article 14 Traceability and Article 15 Notification of Serious Adverse Reactions and Events of EU Directive 200298ECEmhemed Amer TabibОценок пока нет
- ID Faktor Yang Memengaruhi Episode TransfusДокумент6 страницID Faktor Yang Memengaruhi Episode TransfusRahma WatiОценок пока нет
- Immuno 32 2 04Документ52 страницыImmuno 32 2 04mmarquezsaОценок пока нет
- Hemolytic Disease of The NewbornДокумент16 страницHemolytic Disease of The NewbornStanculescu MarianaОценок пока нет
- BMS3136 Transplantation, Transfusion and Specialist Biochemistry Practicals For Blood GroupingДокумент11 страницBMS3136 Transplantation, Transfusion and Specialist Biochemistry Practicals For Blood Groupingsaby abbyОценок пока нет
- Questionnaire (ISBB)Документ14 страницQuestionnaire (ISBB)Angelo Mercede100% (1)
- Transfusion ReactionsДокумент11 страницTransfusion ReactionsBungas Arisudana50% (2)
- Ratih Sumirat - Kegawatdaruratan Klinik ATLS UpdateДокумент16 страницRatih Sumirat - Kegawatdaruratan Klinik ATLS UpdateRatih Nurdiany SumiratОценок пока нет
- Blood Banking Progress ExamДокумент67 страницBlood Banking Progress ExamlenvycahpdelusaОценок пока нет
- Epic TutДокумент15 страницEpic TutTorgbui Gorni Treve IV100% (2)
- 2017b PDFДокумент1 241 страница2017b PDFArizaldo Enriquez CastroОценок пока нет
- Editorial: A Healthy Donor or Unsuspecting PatientДокумент3 страницыEditorial: A Healthy Donor or Unsuspecting PatientLuis Enrique Tinoco JuradoОценок пока нет
- Pmls 1 Final Exam Reviewer: Clinical Chemistry ContДокумент14 страницPmls 1 Final Exam Reviewer: Clinical Chemistry ContPlant in a PotОценок пока нет
- Transfusion Reactions For NursesДокумент24 страницыTransfusion Reactions For NursesMahaОценок пока нет
- Immuno Hematology 25Документ56 страницImmuno Hematology 25BRITTO12Оценок пока нет
- Bloody Easy PDFДокумент164 страницыBloody Easy PDFJenny JeongОценок пока нет
- Heroes of Medicine Bloodless Surgery - Revista TimeДокумент11 страницHeroes of Medicine Bloodless Surgery - Revista Timejorgeduardo9219Оценок пока нет
- Blood Transfusion Skills Laboratory ChecklistДокумент2 страницыBlood Transfusion Skills Laboratory ChecklistJulius BravoОценок пока нет
- Drug Guideline For Iron Polymaltose InjectionДокумент7 страницDrug Guideline For Iron Polymaltose Injectionmirza_baig_46Оценок пока нет
- ST Jude at Work Pledge CardsДокумент1 страницаST Jude at Work Pledge CardsJamieОценок пока нет
- Neonatal Exchange TransfusionДокумент33 страницыNeonatal Exchange TransfusionedrinsneОценок пока нет