Вам также может понравиться
- Physician Onboarding Manual With Articles Jan 2021Документ52 страницыPhysician Onboarding Manual With Articles Jan 2021Rita StarrittОценок пока нет
- Makali Waswa Student - Heritagehs - Furlough-U3l6 Student GuideДокумент7 страницMakali Waswa Student - Heritagehs - Furlough-U3l6 Student Guideapi-536237767Оценок пока нет
- Sample NCS EMG Report PN2202749Документ10 страницSample NCS EMG Report PN2202749Numan AkramОценок пока нет
- 26 Motor Neuron Diseases (FINAL)Документ5 страниц26 Motor Neuron Diseases (FINAL)kath-kathОценок пока нет
- Lipofer BrochureДокумент2 страницыLipofer BrochurenbpravinОценок пока нет
- NANDA Nursing Diagnosis List 2015-2017Документ5 страницNANDA Nursing Diagnosis List 2015-2017Monika Sarmiento100% (2)
- Action Research Proposal SampleДокумент16 страницAction Research Proposal SamplePede Casing100% (1)
- Health: Worksheet No.1Документ5 страницHealth: Worksheet No.1Bryan John GonzalesОценок пока нет
- Jurnal GBSДокумент26 страницJurnal GBSfajar sugandaОценок пока нет
- Guillain-Barré Syndrome Med Student PresentationДокумент16 страницGuillain-Barré Syndrome Med Student PresentationRon ShenkarОценок пока нет
- p191 PDFДокумент7 страницp191 PDFdessriyaОценок пока нет
- Gullian Barre Syndrome: Department of Pharmacy Practice Kle College of Pharmacy Vidyanagar, HubballiДокумент15 страницGullian Barre Syndrome: Department of Pharmacy Practice Kle College of Pharmacy Vidyanagar, Hubballideepjyoti saikiaОценок пока нет
- Guillen BarreДокумент7 страницGuillen BarreDouglas QuispeОценок пока нет
- Guillain-Barre Syndrome: Practice EssentialsДокумент16 страницGuillain-Barre Syndrome: Practice EssentialsUKMBasketОценок пока нет
- Guillain BarreДокумент12 страницGuillain BarreerikaОценок пока нет
- 2020 Axonal Variants of Guillain-Barré Syndrome - An Update PDFДокумент18 страниц2020 Axonal Variants of Guillain-Barré Syndrome - An Update PDFVladimir BasurtoОценок пока нет
- Neuromusk. Bol.Документ7 страницNeuromusk. Bol.Irfan SkejicОценок пока нет
- New Horizons in Osteoporosis Management: Yasser El MiedanyДокумент903 страницыNew Horizons in Osteoporosis Management: Yasser El Miedanyglennys carelaОценок пока нет
- Guillain Barre SyndromeДокумент6 страницGuillain Barre SyndromeErtania NirmalaОценок пока нет
- Arthritis: Septic Arthritis and Tuberculosis ArthritisДокумент10 страницArthritis: Septic Arthritis and Tuberculosis Arthritistaufikoling100% (1)
- Neurologic Disorder FinalДокумент9 страницNeurologic Disorder FinalMary Reigns BuhatОценок пока нет
- PEARSON VUE 1000 FILE Corrected 11-2017Документ245 страницPEARSON VUE 1000 FILE Corrected 11-2017Dr-Jahanzaib GondalОценок пока нет
- Metabolic Bone DiseaseДокумент41 страницаMetabolic Bone DiseaseVenerandaОценок пока нет
- 3rd Announcement PIN PERDOSSIДокумент34 страницы3rd Announcement PIN PERDOSSIAomc Pin PerdossiОценок пока нет
- Lower Motor Neuron Lesions-1Документ9 страницLower Motor Neuron Lesions-1ajay bhatОценок пока нет
- International Journal of Health Sciences and ResearchДокумент8 страницInternational Journal of Health Sciences and ResearchZhara VidaОценок пока нет
- Guillain-Barré Syndrome: Clinical ManifestationsДокумент7 страницGuillain-Barré Syndrome: Clinical Manifestationseagame gamersОценок пока нет
- Guillain Barrésyndrome (GBS) DisabilityScore NeurologicalScalesДокумент1 страницаGuillain Barrésyndrome (GBS) DisabilityScore NeurologicalScalesSutama ArtaОценок пока нет
- ANCA Associated VasculitisДокумент62 страницыANCA Associated VasculitispoluashokОценок пока нет
- Multiple MS Is Lyme Neuro BorrelioseДокумент8 страницMultiple MS Is Lyme Neuro BorrelioseТатяна ТодороваОценок пока нет
- Micronutrients in Neurology and DiseaseДокумент16 страницMicronutrients in Neurology and DiseaseSrinivas PingaliОценок пока нет
- Microbiome and Diseases: Pathogen Infection: Christine Josenhans and Guntram A. GrasslДокумент22 страницыMicrobiome and Diseases: Pathogen Infection: Christine Josenhans and Guntram A. GrasslÂngela Souza BarroqueiroОценок пока нет
- Ubogu - Inflammatory NeuropathiesДокумент24 страницыUbogu - Inflammatory NeuropathiesMarcelo BedoyaОценок пока нет
- PRESENTED BY: Mir Zeeshan ID NO: 18219 SUBMITTED TO: Dr. Abdul RashadДокумент22 страницыPRESENTED BY: Mir Zeeshan ID NO: 18219 SUBMITTED TO: Dr. Abdul RashadMarrium SiddiquiОценок пока нет
- Diseases of ImmunityДокумент55 страницDiseases of ImmunityMeera ANN AJIОценок пока нет
- 02 AmputationДокумент23 страницы02 AmputationJuanitoCabatañaLimIIIОценок пока нет
- Vasculitis: VASCULITIS Is A Primary Inflammatory Disease Process of The VasculatureДокумент43 страницыVasculitis: VASCULITIS Is A Primary Inflammatory Disease Process of The VasculaturelihayatiОценок пока нет
- Clinical PracticeДокумент13 страницClinical PracticeAnonymous vnv6QFОценок пока нет
- Approach To AtaxiaДокумент6 страницApproach To AtaxiaVivek KumarОценок пока нет
- 2021 JAMA Diagnosis and Treatment of Multiple Sclerosis A ReviewДокумент15 страниц2021 JAMA Diagnosis and Treatment of Multiple Sclerosis A ReviewItz Hernandez GarciaОценок пока нет
- Osteo Arthit IsДокумент19 страницOsteo Arthit IsShaa ShawalishaОценок пока нет
- Lumbarspinalstenosisin Olderadults: Anna M. Lafian,, Karina D. TorralbaДокумент12 страницLumbarspinalstenosisin Olderadults: Anna M. Lafian,, Karina D. TorralbaIhsan KОценок пока нет
- An Overview of Autoimmune and Paraneoplastic EncefaliteДокумент14 страницAn Overview of Autoimmune and Paraneoplastic Encefaliterafael rocha novaesОценок пока нет
- Systemic Lupus ErythematosusДокумент40 страницSystemic Lupus ErythematosusAkshan SentinelОценок пока нет
- Harrison TablesДокумент163 страницыHarrison TablesPratikОценок пока нет
- Nerve InjuryДокумент16 страницNerve InjuryPasupathy PalaniappanОценок пока нет
- (Upgraded) Damage Control Orthopaedics DR Bambang SpOTДокумент37 страниц(Upgraded) Damage Control Orthopaedics DR Bambang SpOTroroОценок пока нет
- Cardio Respiratory Asessment For PhysiotДокумент10 страницCardio Respiratory Asessment For PhysiotJayden HiiОценок пока нет
- Motor Neuron DiseaseДокумент7 страницMotor Neuron DiseasegeraldineongОценок пока нет
- Sci RehabДокумент45 страницSci RehabkaushikawebОценок пока нет
- Progressive Myoclonic Epilepsies - Practical Neurology 2015. MalekДокумент8 страницProgressive Myoclonic Epilepsies - Practical Neurology 2015. MalekchintanОценок пока нет
- DystoniaДокумент24 страницыDystoniaAyesha NasirОценок пока нет
- J Neuroscience 2016 05 057 PDFДокумент21 страницаJ Neuroscience 2016 05 057 PDFpedroОценок пока нет
- Gulian Barre SyndromeДокумент12 страницGulian Barre SyndromeShauki AliОценок пока нет
- Cell-Based Therapy To Reduce Mortality From COVID-19Документ16 страницCell-Based Therapy To Reduce Mortality From COVID-19Chelsea Shannen Marie CarreonОценок пока нет
- Metabolic Bone DisordersДокумент24 страницыMetabolic Bone Disordersbpt20% (1)
- Review On Molecular Epidemiology and Public Health Significance of BrucellosisДокумент11 страницReview On Molecular Epidemiology and Public Health Significance of BrucellosiseduardoОценок пока нет
- Madelung's Deformity of The Wrist-CurrentДокумент4 страницыMadelung's Deformity of The Wrist-CurrentAnonymous bUBXIFfОценок пока нет
- Child Abuse and Neglect-Dr - Anisha NandaДокумент49 страницChild Abuse and Neglect-Dr - Anisha NandaHaripriya SukumarОценок пока нет
- Anesthesia & Clinical Care: HSOA Journal ofДокумент6 страницAnesthesia & Clinical Care: HSOA Journal ofHerald Scholarly Open Access100% (1)
- Carbohydrate MetabolismДокумент53 страницыCarbohydrate Metabolismjehram navalesОценок пока нет
- Fmed 08 697986Документ14 страницFmed 08 697986sana siddiqueОценок пока нет
- Spinal Tumors - A Brief OverviewДокумент38 страницSpinal Tumors - A Brief OverviewRAVIRAJ GHORPADE BELGAUM ADVANCED NEUROSURGERYОценок пока нет
- Clinical Training Profile:: PhysiotherapyДокумент17 страницClinical Training Profile:: Physiotherapyrenata miateliОценок пока нет
- End of Term 3 Musomhs Cat MCQ July 2020-1Документ16 страницEnd of Term 3 Musomhs Cat MCQ July 2020-1MustafaОценок пока нет
- Guillain Barre SyndromeДокумент170 страницGuillain Barre SyndromeAfra HanifiОценок пока нет
- NeuromusculardiseaseДокумент24 страницыNeuromusculardiseasem3510Оценок пока нет
- Terminology of Mechanical Injuries: The Birmingham Eye Trauma Terminology (BETT)Документ10 страницTerminology of Mechanical Injuries: The Birmingham Eye Trauma Terminology (BETT)febyrahmaОценок пока нет
- Myesthenia GravisДокумент16 страницMyesthenia Gravism3510Оценок пока нет
- Sandoz Sertraline: Sertraline Hydrochloride 25 MG, 50 MG and 100 MG CapsulesДокумент1 страницаSandoz Sertraline: Sertraline Hydrochloride 25 MG, 50 MG and 100 MG Capsulesm3510Оценок пока нет
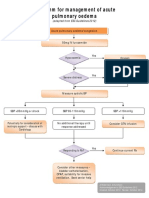
- Algorithm For Management of Acute Pulmonary Oedema PDFДокумент1 страницаAlgorithm For Management of Acute Pulmonary Oedema PDFm3510Оценок пока нет
- AAI Scholarships Policy Handbook 2016Документ124 страницыAAI Scholarships Policy Handbook 2016boni_sebayangОценок пока нет
- University Hosp. Kings County Hosp. Brookdale Maimonides Coney IslandДокумент1 страницаUniversity Hosp. Kings County Hosp. Brookdale Maimonides Coney Islandm3510Оценок пока нет
- Komuter SurabayaДокумент1 страницаKomuter SurabayaYopi MagfirudinОценок пока нет
- Havrix VaksinДокумент16 страницHavrix Vaksinm3510Оценок пока нет
- Havrix VaksinДокумент16 страницHavrix Vaksinm3510Оценок пока нет
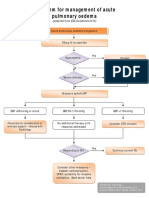
- Algorithm For Management of Acute Pulmonary Oedema PDFДокумент1 страницаAlgorithm For Management of Acute Pulmonary Oedema PDFm3510Оценок пока нет
- Swot Analysis: BERNARDO, Eleina Bea L. 11 Grade - Plato of Athens (ABM)Документ4 страницыSwot Analysis: BERNARDO, Eleina Bea L. 11 Grade - Plato of Athens (ABM)Eleina Bea BernardoОценок пока нет
- Biotechnoloy Benefits and Biotechnology As An Interdisciplinary Field. ROLL#31 MANAL (M.SC FINAL)Документ16 страницBiotechnoloy Benefits and Biotechnology As An Interdisciplinary Field. ROLL#31 MANAL (M.SC FINAL)Manal Shakeel RajputОценок пока нет
- Ear MedicationДокумент15 страницEar MedicationPascalina Monts'onyaneОценок пока нет
- D'Amico Risk ClassificationДокумент6 страницD'Amico Risk ClassificationStirОценок пока нет
- Mnemonics PDFДокумент10 страницMnemonics PDFود امدرОценок пока нет
- Spike DetoxДокумент2 страницыSpike Detoxrptitalia courses & sessionsОценок пока нет
- Health 6 - Q1 - DW1Документ3 страницыHealth 6 - Q1 - DW1Mark Patrics VerderaОценок пока нет
- 2018 Persistent DiarrhoeaДокумент8 страниц2018 Persistent DiarrhoeaDanielaRojasОценок пока нет
- Letters Re S. 975 Gov. DHEC EMD - 3.13.24Документ10 страницLetters Re S. 975 Gov. DHEC EMD - 3.13.24MyrtleBeachSC newsОценок пока нет
- People's Judgments of Human and Robot Behaviors: A Robust Set of Behaviors and Some DiscrepanciesДокумент3 страницыPeople's Judgments of Human and Robot Behaviors: A Robust Set of Behaviors and Some DiscrepanciesShahid KhanОценок пока нет
- Childhood Autism Rating Scale, 2Nd Edition (Cars2)Документ4 страницыChildhood Autism Rating Scale, 2Nd Edition (Cars2)Khadidja BoutouilОценок пока нет
- Geriatrics, Gerontology, GeronticДокумент5 страницGeriatrics, Gerontology, GeronticTsaabitah AnwarОценок пока нет
- Draft Narrative ReportДокумент8 страницDraft Narrative ReportChristine DiloyОценок пока нет
- Master Thesis Product ManagementДокумент7 страницMaster Thesis Product Managementjjvveqvcf100% (2)
- Project NewДокумент31 страницаProject NewDrGajanan VaishnavОценок пока нет
- Screen TIme Soap NotesДокумент3 страницыScreen TIme Soap NotesAva JonesОценок пока нет
- National Health Mission (NHM) : Kavita Singh, Director - FinanceДокумент64 страницыNational Health Mission (NHM) : Kavita Singh, Director - FinanceOWAIS ZAHOOR BHATОценок пока нет
- Personality and Individual Di FferencesДокумент7 страницPersonality and Individual Di FferencesDarojaturroofi'ah SodiqОценок пока нет
- Handout 1Документ4 страницыHandout 1Namja Ileum Ozara GaabucayanОценок пока нет
- Bibliograhy-Tanishka MistryДокумент23 страницыBibliograhy-Tanishka Mistryapi-512047026Оценок пока нет
- Audrey Sanders: Cosmetology (August 2022)Документ2 страницыAudrey Sanders: Cosmetology (August 2022)api-618098519Оценок пока нет
- Arc Flash Training - Electrical Safety Training in The Workplace - Lock Out TrainingДокумент6 страницArc Flash Training - Electrical Safety Training in The Workplace - Lock Out TrainingJemeraldОценок пока нет
- Rammed Earth: Y18AP0107 Y18AP0111 Y18AP0112 Y18AP0114 Y18AP0115Документ15 страницRammed Earth: Y18AP0107 Y18AP0111 Y18AP0112 Y18AP0114 Y18AP0115Harsha Vardhan KattaОценок пока нет
- Movement Competency TrainingДокумент50 страницMovement Competency TrainingPrincess Meth Catubigan SarominesОценок пока нет