Вам также может понравиться
- Hyperthyroidism 2011Документ30 страницHyperthyroidism 2011Elyza MagsaysayОценок пока нет
- The Endocrine System Uses Chemical Messengers Called HormonesДокумент6 страницThe Endocrine System Uses Chemical Messengers Called HormonesLuiciaОценок пока нет
- HypothyroidismДокумент2 страницыHypothyroidismDanteAndreiОценок пока нет
- GOITERДокумент4 страницыGOITERJerika Shane MañosoОценок пока нет
- Dietary Management in FeverДокумент77 страницDietary Management in FeverJoniya GalbaoОценок пока нет
- ITP (Idiopathic Thrombocytopenic Purpura)Документ20 страницITP (Idiopathic Thrombocytopenic Purpura)Iqra NaseemОценок пока нет
- Worksheet On Exercise No. 7 Case Study On Diabetes MellitusДокумент10 страницWorksheet On Exercise No. 7 Case Study On Diabetes MellitusShannen CostoОценок пока нет
- Primary Health CareДокумент11 страницPrimary Health CareDanica ZaragozaОценок пока нет
- Causes of HypothyroidismДокумент6 страницCauses of HypothyroidismIsabel Castillo100% (1)
- TBL (Miscarrriage)Документ36 страницTBL (Miscarrriage)hitsugayat_7100% (1)
- SEPTICARTHRITISДокумент2 страницыSEPTICARTHRITISapi-3822433Оценок пока нет
- Case Study - Nephrotic SyndromeДокумент42 страницыCase Study - Nephrotic Syndromefarmasi rsud cilincingОценок пока нет
- Case Presentation Og HyperthyroidismДокумент7 страницCase Presentation Og HyperthyroidismMegan Mendoza0% (2)
- HyperthyroidismДокумент40 страницHyperthyroidismmypublicidОценок пока нет
- Nausea VomitingДокумент36 страницNausea VomitingDian Fitri100% (1)
- Addison' S Disease: Case PresentationДокумент34 страницыAddison' S Disease: Case PresentationShane Olanosa PillonarОценок пока нет
- Non-Toxic GoiterДокумент17 страницNon-Toxic Goiterabigaille chua100% (1)
- Adrenal DisordersДокумент48 страницAdrenal DisordersMubeenUrRehmanОценок пока нет
- HypothyroidismДокумент5 страницHypothyroidismlikeaquarianОценок пока нет
- NafldДокумент30 страницNafldprabhatguyОценок пока нет
- Piyas Utsav ProgramДокумент4 страницыPiyas Utsav ProgramdrmbalarОценок пока нет
- Graves DseДокумент5 страницGraves DseHester Marie SimpiaОценок пока нет
- Thyroid Function TestsДокумент21 страницаThyroid Function TestsPraneeth TirumalasettyОценок пока нет
- Philippine Urological Association, Inc.: Executive Committee and Board Members 1997Документ12 страницPhilippine Urological Association, Inc.: Executive Committee and Board Members 1997mits98Оценок пока нет
- Anti-Gout DrugsДокумент38 страницAnti-Gout Drugsapi-306036754Оценок пока нет
- Vaccination Chart: National Immunization Schedule For New BornДокумент20 страницVaccination Chart: National Immunization Schedule For New BornsmilealwplzОценок пока нет
- Patient ProfileДокумент9 страницPatient ProfileValarmathiОценок пока нет
- Malabsorption SyndromeДокумент24 страницыMalabsorption SyndromeanojanОценок пока нет
- 10 Aschool Health PRGRM DoneДокумент166 страниц10 Aschool Health PRGRM DoneHarshitha100% (1)
- NCM116 Addison DiseaseДокумент20 страницNCM116 Addison DiseaseSofia MikaelaОценок пока нет
- 4-Systematic Surgery Abdominal HerniaДокумент44 страницы4-Systematic Surgery Abdominal HerniaabdisamedОценок пока нет
- Promoting Nutritional Health During Pregnancy 19-20Документ25 страницPromoting Nutritional Health During Pregnancy 19-20Tony KhattarОценок пока нет
- Hydatidiform Mole - OverviewДокумент4 страницыHydatidiform Mole - Overviewannmanalad9438Оценок пока нет
- Celiac Disease Gluten Related DisordersДокумент49 страницCeliac Disease Gluten Related Disordersxaviermargarida100% (1)
- Health Talk - Diabetes MellitusДокумент57 страницHealth Talk - Diabetes MellitusRimel Dizon EvaristoОценок пока нет
- Role of Food and Exercise in Polycystic Ovarian SyndromeДокумент3 страницыRole of Food and Exercise in Polycystic Ovarian SyndromeInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- Cushing's SyndromeДокумент25 страницCushing's SyndromeRahmah Shah BahaiОценок пока нет
- PoliomyelitisДокумент13 страницPoliomyelitiscasandra morante100% (2)
- HIV Treatment 2Документ3 страницыHIV Treatment 2kimglaidyl bontuyanОценок пока нет
- Food AdulterationДокумент13 страницFood Adulterationramanjeet kaurОценок пока нет
- Fat Soluble VitaminsДокумент63 страницыFat Soluble Vitaminsmariah marОценок пока нет
- SAMДокумент108 страницSAMAlimyon Abilar MontoloОценок пока нет
- Hypothyroidism: Darien Liew DaojuinДокумент41 страницаHypothyroidism: Darien Liew DaojuinDarien LiewОценок пока нет
- Diabetes MellitusДокумент93 страницыDiabetes MellitusAllen Reyes SantosОценок пока нет
- Addison's DiseaseДокумент9 страницAddison's Diseaseash ashОценок пока нет
- Ferrous Sulfate: Generic NameДокумент3 страницыFerrous Sulfate: Generic NamefahadОценок пока нет
- Convulsive Disorders in ChildrenДокумент44 страницыConvulsive Disorders in ChildrenMurugesanОценок пока нет
- Mfe, Ferrous Sulfate, Calcium Drug StudyДокумент3 страницыMfe, Ferrous Sulfate, Calcium Drug StudyMary Shane MoraldeОценок пока нет
- Ablilasha Ashish Divya Gayatri Sarita Shrutika:: Presented byДокумент52 страницыAblilasha Ashish Divya Gayatri Sarita Shrutika:: Presented bysashk_lucky21100% (1)
- Pituitary Adenoma Concept MapДокумент1 страницаPituitary Adenoma Concept Mapnursing concept mapsОценок пока нет
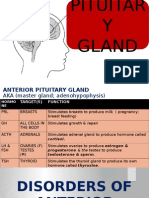
- Disorders of Pituitary GlandДокумент34 страницыDisorders of Pituitary GlandninaaltheaОценок пока нет
- Menopause Hormone Replacement TherapyДокумент4 страницыMenopause Hormone Replacement Therapybidan22Оценок пока нет
- Diabetes Mellitus and PregnancyДокумент45 страницDiabetes Mellitus and Pregnancyilham muntari100% (1)
- Thyroid Function TestДокумент11 страницThyroid Function TestBookmyscansОценок пока нет
- Abnormal Thyroid Function A Practical ApproachДокумент111 страницAbnormal Thyroid Function A Practical ApproachGepengCungkring100% (1)
- Hyperthyroidism and HypothyroidismДокумент59 страницHyperthyroidism and HypothyroidismJun AmaroОценок пока нет
- Hyper BrochureДокумент2 страницыHyper BrochureVksudhar SanamОценок пока нет
- Diabetes Mellitus: Dr. Madhusudan SwarnkarДокумент45 страницDiabetes Mellitus: Dr. Madhusudan Swarnkarmadhusudan swarnkarОценок пока нет
- Study Guide For NURS 320 Exam 2Документ15 страницStudy Guide For NURS 320 Exam 2Anthony Del RioОценок пока нет
- Ophthalmia NeonatorumДокумент12 страницOphthalmia NeonatorumDemewoz Fikir100% (2)
- Diabetes Mellitus MDДокумент5 страницDiabetes Mellitus MDDemewoz FikirОценок пока нет
- Neonatal SepsisДокумент63 страницыNeonatal SepsisDemewoz Fikir100% (2)
- Congenital Adrenal Hyperplasia JohnДокумент48 страницCongenital Adrenal Hyperplasia JohnDemewoz FikirОценок пока нет
- Theater InstallationДокумент7 страницTheater InstallationtemamОценок пока нет
- Andre Bazin, The Ontology of The Photographic Image From His Book What Is Cinema Vol. IДокумент8 страницAndre Bazin, The Ontology of The Photographic Image From His Book What Is Cinema Vol. IAnkit LadiaОценок пока нет
- School Earthquake Preparedness Evaluation FormДокумент2 страницыSchool Earthquake Preparedness Evaluation FormAdrin Mejia75% (4)
- Xafsa 1Документ19 страницXafsa 1Heitham OmarОценок пока нет
- Former Rajya Sabha MP Ajay Sancheti Appeals Finance Minister To Create New Laws To Regulate Cryptocurrency MarketДокумент3 страницыFormer Rajya Sabha MP Ajay Sancheti Appeals Finance Minister To Create New Laws To Regulate Cryptocurrency MarketNation NextОценок пока нет
- Kalbelia Dance Rajasthan - Kalbelia Rajasthani Folk Dance KalbeliaДокумент6 страницKalbelia Dance Rajasthan - Kalbelia Rajasthani Folk Dance KalbeliarahulgabdaОценок пока нет
- Satellite Value Chain: Snapshot 2017Документ13 страницSatellite Value Chain: Snapshot 2017syrijal26Оценок пока нет
- Fastener Torque Charts: Phone: 1-800-558-2808 Fax: 1-800-553-8769Документ2 страницыFastener Torque Charts: Phone: 1-800-558-2808 Fax: 1-800-553-8769KOMATSU SHOVELОценок пока нет
- 3.6 A 40Nm Cmos Highly Linear 0.4-To-6Ghz Receiver Resilient To 0Dbm Out-Of-Band BlockersДокумент3 страницы3.6 A 40Nm Cmos Highly Linear 0.4-To-6Ghz Receiver Resilient To 0Dbm Out-Of-Band Blockershaoyue huangОценок пока нет
- ErtlДокумент64 страницыErtlManpreet SinghОценок пока нет
- Boonton Radio Corporation - The Notebook 12Документ8 страницBoonton Radio Corporation - The Notebook 12Luiz Roberto PascotteОценок пока нет
- Symantec Endpoint Protection 14.3 RU3 Release NotesДокумент28 страницSymantec Endpoint Protection 14.3 RU3 Release NotesMilind KuleОценок пока нет
- 1422-Article Text-3684-1-10-20211104Документ57 страниц1422-Article Text-3684-1-10-20211104f.kpobi1473Оценок пока нет
- Far Eastern University Mba - Thesis 060517Документ2 страницыFar Eastern University Mba - Thesis 060517Lex AcadsОценок пока нет
- Project Report - Performance Anaylysis of Mutual Funds in IndiaДокумент52 страницыProject Report - Performance Anaylysis of Mutual Funds in Indiapankaj100% (1)
- Jim 1000 RC 3Документ33 страницыJim 1000 RC 3singingblueeОценок пока нет
- Basic Elements of The Communication ProcessДокумент13 страницBasic Elements of The Communication ProcessMech JTubao67% (3)
- Effect of Social Economic Factors On Profitability of Soya Bean in RwandaДокумент7 страницEffect of Social Economic Factors On Profitability of Soya Bean in RwandaMarjery Fiona ReyesОценок пока нет
- Republic of The Philippines Department of Education Deped Complex, Pasig City Science Iii K To 12 Curriculum Guide Planner / Budget of WorkДокумент3 страницыRepublic of The Philippines Department of Education Deped Complex, Pasig City Science Iii K To 12 Curriculum Guide Planner / Budget of WorkLedie Lou Cetoy SuperalesОценок пока нет
- Cel2106 SCL Worksheet 6Документ3 страницыCel2106 SCL Worksheet 6HarryJoy JackОценок пока нет
- CH 6 Answers (All) PDFДокумент29 страницCH 6 Answers (All) PDFAhmed SideegОценок пока нет
- Hunk (Aakc) - (Nov 2015)Документ68 страницHunk (Aakc) - (Nov 2015)Russell RiderОценок пока нет
- Thesis Final 2 Number c1-c5Документ167 страницThesis Final 2 Number c1-c5Kimverly DomaganОценок пока нет
- The Mystery of Putins DissertationДокумент16 страницThe Mystery of Putins DissertationDoinaCebanuОценок пока нет
- Prototyping: by DR Sampa Unnikrishnan Yateer Creative Solutions Reachus@Yateer - In, 8971442777Документ70 страницPrototyping: by DR Sampa Unnikrishnan Yateer Creative Solutions Reachus@Yateer - In, 8971442777ShivashankarОценок пока нет
- Accomplishment Report Filipino Values MonthДокумент4 страницыAccomplishment Report Filipino Values MonthIan Santos B. Salinas100% (10)
- Arch Plan-Agner Boco (For Blue Print) - p1Документ1 страницаArch Plan-Agner Boco (For Blue Print) - p1Jay CeeОценок пока нет
- Comparative Analysis of State Bank of India With Other Credit SchemesДокумент97 страницComparative Analysis of State Bank of India With Other Credit SchemesVKM2013Оценок пока нет
- Perfil Clinico de Pacientes Con Trastornos de La Conducta AlimentariaДокумент44 страницыPerfil Clinico de Pacientes Con Trastornos de La Conducta AlimentariaFrida PandoОценок пока нет
- Ga2 27:6:23Документ1 страницаGa2 27:6:23john HuntОценок пока нет