Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
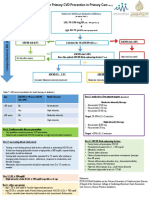
- Dyslipidemia Final Poster June 24Документ2 страницыDyslipidemia Final Poster June 24drabdulrabbОценок пока нет
- Pcos TreatmentДокумент13 страницPcos TreatmentAnonymous PuaFsusОценок пока нет
- DigoxinДокумент2 страницыDigoxinIsabel Barredo Del MundoОценок пока нет
- Drug StudyДокумент4 страницыDrug StudySharwen_R_Rome_5572Оценок пока нет
- Mufia Muin, Prema Hapsari Hidayati, Indah Lestari, Gina Isni D Iskandar, Nurul Faiqah, Agung SukriadiДокумент5 страницMufia Muin, Prema Hapsari Hidayati, Indah Lestari, Gina Isni D Iskandar, Nurul Faiqah, Agung SukriadimufiaОценок пока нет
- Daftar PustakaДокумент2 страницыDaftar PustakaReza Ridho PahleviОценок пока нет
- Ascvd PrimaryДокумент30 страницAscvd PrimarykunkkonkОценок пока нет
- AmlodipineДокумент22 страницыAmlodipineBetaОценок пока нет
- 11) Drugs Used in DyslipidemiasДокумент8 страниц11) Drugs Used in Dyslipidemiasفاعل خيرОценок пока нет
- Pharmacology QuestionsДокумент15 страницPharmacology QuestionsAnant KhotОценок пока нет
- Name That MedicineДокумент1 страницаName That Medicinegolden fleeceОценок пока нет
- Pharmacology Notes NursingДокумент25 страницPharmacology Notes NursingKyle Marks100% (5)
- The Effectiveness of Psidium Guajava Leaf Tea AsДокумент26 страницThe Effectiveness of Psidium Guajava Leaf Tea AsDanica Nicole Seco GabonОценок пока нет
- LocholДокумент6 страницLocholKashif FarooquiОценок пока нет
- Cardiology Pharmacology Review: Dhiren Patel, Pharmd, CdeДокумент74 страницыCardiology Pharmacology Review: Dhiren Patel, Pharmd, Cdeshannon_marrero_1Оценок пока нет
- Chemistry in The Pharmaceutical IndustryДокумент27 страницChemistry in The Pharmaceutical IndustryUsi Nur PamilianiОценок пока нет
- Open Letter To FDA On Its Response To MRC's Citizen Petition RE The Vascepa SNDAДокумент56 страницOpen Letter To FDA On Its Response To MRC's Citizen Petition RE The Vascepa SNDAMedical Research Collaborative, LLCОценок пока нет
- Dangers of Statin DrugsДокумент17 страницDangers of Statin Drugslijyonas100% (2)
- Medical App DislipidemiaДокумент59 страницMedical App DislipidemiaCecilia Casandra UneputtyОценок пока нет
- The Pathological Effects of Hyperglycaemia On The Cardiovascular (CV) System and BrainДокумент5 страницThe Pathological Effects of Hyperglycaemia On The Cardiovascular (CV) System and BrainRyzka Izza MayFanyОценок пока нет
- Ellison - Hidden Truth About Cholesterol-Lowering Drugs (2006) PDFДокумент42 страницыEllison - Hidden Truth About Cholesterol-Lowering Drugs (2006) PDFridwansurono100% (2)
- This Content Downloaded From 103.251.182.254 On Sat, 18 Jan 2020 04:52:17 UTCДокумент9 страницThis Content Downloaded From 103.251.182.254 On Sat, 18 Jan 2020 04:52:17 UTCsinnanancyОценок пока нет
- ACC Phamrmacology PDFДокумент100 страницACC Phamrmacology PDFElva SorumbaОценок пока нет
- Drug-Food Interactions: DR - Kawooya Francis, Pharmd, MpsДокумент28 страницDrug-Food Interactions: DR - Kawooya Francis, Pharmd, MpsNina100% (2)
- Nutrition and Stroke PreventionДокумент6 страницNutrition and Stroke PreventionNhat NamОценок пока нет
- Drug Nutrient Depletions - Interactions ChartДокумент2 страницыDrug Nutrient Depletions - Interactions ChartEygenia PapadpoulouОценок пока нет
- New Developments in The Management of DyslipidemiaДокумент63 страницыNew Developments in The Management of DyslipidemiaM Azmi HОценок пока нет
- Drug StudyДокумент12 страницDrug StudyErvin Kyle Osmeña100% (1)
- Coronary Heart Disease Seondary Prevention - Review ArticleДокумент12 страницCoronary Heart Disease Seondary Prevention - Review ArticleqanitaОценок пока нет
- Drug Study (Simvastatin)Документ2 страницыDrug Study (Simvastatin)Julianne Jeaven Bumanglag LimОценок пока нет