
Вам также может понравиться
- Stilpane Comb Tab Za Stiltab 1204 03 Epi 2020.03.09-1Документ16 страницStilpane Comb Tab Za Stiltab 1204 03 Epi 2020.03.09-1allan.prathipati07Оценок пока нет
- Drug StudyДокумент4 страницыDrug Studymisstheatricality130Оценок пока нет
- ParacetamolДокумент5 страницParacetamolunimintt100% (1)
- The Influence of Hepatic Disorders On Drug DispositionДокумент14 страницThe Influence of Hepatic Disorders On Drug DispositionMelinda AriniОценок пока нет
- Drug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineДокумент21 страницаDrug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineAtakan Yeşil100% (1)
- Clinical Pharmacology, Toxicology and Poisoning: 1. Drug Metabolism and InteractionsДокумент26 страницClinical Pharmacology, Toxicology and Poisoning: 1. Drug Metabolism and InteractionsNadia Ancharuz100% (1)
- Drug StudyДокумент9 страницDrug StudyOdarp PradzОценок пока нет
- Furosemide Tables:: Pharmacokinetics Bioavailability Peak Plasma Level Plasma Half-Life Active Metabolites EliminationДокумент4 страницыFurosemide Tables:: Pharmacokinetics Bioavailability Peak Plasma Level Plasma Half-Life Active Metabolites Eliminationmole_fkОценок пока нет
- Diuretics: Generic Name: FUROSEMIDEДокумент12 страницDiuretics: Generic Name: FUROSEMIDEJR BetonioОценок пока нет
- Medfact Pocket Guide Drug Interaction: FurosemideДокумент7 страницMedfact Pocket Guide Drug Interaction: FurosemideParis Yayuk JacksonОценок пока нет
- Enzyme Inducers and Inhibitors TransДокумент6 страницEnzyme Inducers and Inhibitors TransLeonallee MayorОценок пока нет
- Drug StudyДокумент3 страницыDrug StudyGail SantosОценок пока нет
- Lecture 22. Drugs Used in Renal and Urinary Tract DisordersДокумент38 страницLecture 22. Drugs Used in Renal and Urinary Tract DisorderskrisnadewirahadiОценок пока нет
- Drug InteractionДокумент11 страницDrug InteractionHashim MohammedОценок пока нет
- Drug Study Medcor AguinaldoДокумент6 страницDrug Study Medcor AguinaldoYana PotОценок пока нет
- Liver CirrhosisДокумент39 страницLiver CirrhosisДенис КовшОценок пока нет
- Icu Drug StudyДокумент7 страницIcu Drug StudyHazel Palomares100% (1)
- Drug InteractionsДокумент27 страницDrug InteractionsIndu Sri100% (4)
- Drugs StudyДокумент35 страницDrugs StudyMark CapillanesОценок пока нет
- M3 - Lesson 1bДокумент20 страницM3 - Lesson 1bLhara MañoОценок пока нет
- 2022 Oxford Handbook of Anaesthesia Oxford Press 5th Edition ExportДокумент2 страницы2022 Oxford Handbook of Anaesthesia Oxford Press 5th Edition ExportHany Elbarougy0% (1)
- MalariaДокумент45 страницMalariaSiya PatelОценок пока нет
- Drug Name Dose, Route, Frequency Mechanism of Drug Indications Adverse Effects Contraindications Nursing ResponsibilitiesДокумент15 страницDrug Name Dose, Route, Frequency Mechanism of Drug Indications Adverse Effects Contraindications Nursing ResponsibilitiesitsmechachaОценок пока нет
- Antihypertensive AgentsДокумент33 страницыAntihypertensive AgentsJuwairia tariqОценок пока нет
- PHRM 465 Pre-Class HandoutДокумент5 страницPHRM 465 Pre-Class Handoutapi-649060644Оценок пока нет
- Summary of Product Characteristics 1 Name of The Medicinal ProductДокумент9 страницSummary of Product Characteristics 1 Name of The Medicinal Productddandan_2Оценок пока нет
- Drug Induced Hyperuricemia GoutДокумент3 страницыDrug Induced Hyperuricemia GoutAnggun Cahya MertyanaОценок пока нет
- Non-Steroidal Anti-Inflammatory DrugsДокумент25 страницNon-Steroidal Anti-Inflammatory DrugsSanchit MehanОценок пока нет
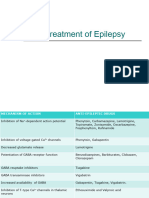
- Drug Treatment of EpilepsyДокумент81 страницаDrug Treatment of EpilepsyAnifowose SamsonОценок пока нет
- Drug Study - CholangioДокумент10 страницDrug Study - CholangioClaireMutiaОценок пока нет
- Proses F.kinetik-F.dinamik Ppds 2017Документ33 страницыProses F.kinetik-F.dinamik Ppds 2017intan purnamaОценок пока нет
- PharmaДокумент1 страницаPharmaARVIN ZUBIAGAОценок пока нет
- Cortex Where Spread of SeizureДокумент11 страницCortex Where Spread of SeizureDustin JohnОценок пока нет
- HEMOdrug Study (Jul 2013)Документ7 страницHEMOdrug Study (Jul 2013)Leoni HerreraОценок пока нет
- Ultimate Pre-Reg BNF NotesДокумент29 страницUltimate Pre-Reg BNF NotesBob100% (7)
- Adverse Drug Reactions and Drug InteractionsДокумент10 страницAdverse Drug Reactions and Drug Interactions88AKKОценок пока нет
- Antiepileptics PD 501Документ27 страницAntiepileptics PD 501SidraОценок пока нет
- Drugs Coronary Ward IIДокумент7 страницDrugs Coronary Ward IITimothy Joy VercelesОценок пока нет
- Drugs and Kidney DiseasesДокумент46 страницDrugs and Kidney Diseasesمرتضى محمد فاضل جرجوكОценок пока нет
- Drug-Study PharmacologyДокумент11 страницDrug-Study PharmacologyEmmanuel CaracalОценок пока нет
- Adverse Drug Reaction: Muhammad Faisal NadeemДокумент65 страницAdverse Drug Reaction: Muhammad Faisal NadeemfaisalnadeemОценок пока нет
- Mefenamic Acid Is A Non-SteroidalДокумент4 страницыMefenamic Acid Is A Non-SteroidalAnkan PalОценок пока нет
- Acute Poisoning of Therapeutic Agents: by Alemayehu TomaДокумент42 страницыAcute Poisoning of Therapeutic Agents: by Alemayehu TomaYohannis AsefaОценок пока нет
- Anaesthesia in CKD MAJUДокумент21 страницаAnaesthesia in CKD MAJUAnonymous BQM9271ZXОценок пока нет
- Drug Metabolism and Excretion by AsadДокумент19 страницDrug Metabolism and Excretion by AsadAsadullah ghalibОценок пока нет
- Mefenamic Acid Drug ProfileДокумент3 страницыMefenamic Acid Drug ProfileAhmad WaliОценок пока нет
- Drug Induced Liver Diseases (DILD) : M. DeepalakshmiДокумент22 страницыDrug Induced Liver Diseases (DILD) : M. DeepalakshmicrissОценок пока нет
- LM, KLДокумент5 страницLM, KLVictor CondeОценок пока нет
- Pharmacology Test 3 ReviewДокумент6 страницPharmacology Test 3 ReviewNatalia BortellОценок пока нет
- Drugs & KidneyДокумент18 страницDrugs & KidneyAamir MohammadОценок пока нет
- Prescribing in Liver Disease Issue 2 Volume 32 Australian PrescriberДокумент6 страницPrescribing in Liver Disease Issue 2 Volume 32 Australian PrescriberAnonymous 9dVZCnTXSОценок пока нет
- Introduction To Drug InteractionsДокумент19 страницIntroduction To Drug InteractionsPyara MunnaОценок пока нет
- Antidyslipidemic Drugs (Geppetti)Документ32 страницыAntidyslipidemic Drugs (Geppetti)Ariel OlshevskyОценок пока нет
- Endocrine DrugsДокумент6 страницEndocrine DrugsdiriniumОценок пока нет
- Drugs Acting On Gastrointestinal SystemДокумент41 страницаDrugs Acting On Gastrointestinal SystemDivya JoyОценок пока нет
- Acute Renal FailureДокумент33 страницыAcute Renal Failureimranqazi11Оценок пока нет
- Dietary Interventions in Liver Disease: Foods, Nutrients, and Dietary SupplementsОт EverandDietary Interventions in Liver Disease: Foods, Nutrients, and Dietary SupplementsРейтинг: 5 из 5 звезд5/5 (1)
- Basic Pharmacology And Drug Calculations [Practice Questions And Answers]От EverandBasic Pharmacology And Drug Calculations [Practice Questions And Answers]Рейтинг: 4 из 5 звезд4/5 (1)
- Pharmacology of SulphonamidesДокумент21 страницаPharmacology of SulphonamidesGANESH KUMAR JELLA100% (1)
- PharmacosomeДокумент17 страницPharmacosomeGANESH KUMAR JELLAОценок пока нет
- New Drug Application HardДокумент37 страницNew Drug Application HardGANESH KUMAR JELLA100% (1)
- Medicinal PlantsДокумент29 страницMedicinal PlantsGANESH KUMAR JELLAОценок пока нет
- Liposome Drug Delivery SystemДокумент28 страницLiposome Drug Delivery SystemGANESH KUMAR JELLA100% (1)
- Dissolution ApparatusДокумент29 страницDissolution ApparatusGANESH KUMAR JELLA75% (4)
- MacrolidesДокумент25 страницMacrolidesGANESH KUMAR JELLA100% (3)
- Good Clinical Practice Guidelines: A Seminar OnДокумент55 страницGood Clinical Practice Guidelines: A Seminar OnGANESH KUMAR JELLAОценок пока нет
- GMP GuidelinesДокумент40 страницGMP GuidelinesGANESH KUMAR JELLA100% (2)
- Cology of Pediatrics N GeriatricsДокумент41 страницаCology of Pediatrics N GeriatricsGANESH KUMAR JELLA100% (1)
- Floating Drug Delivery SystemДокумент27 страницFloating Drug Delivery SystemGANESH KUMAR JELLA100% (1)
- Drug Distribution: Visit For More Ppt's & MaterialДокумент26 страницDrug Distribution: Visit For More Ppt's & MaterialGANESH KUMAR JELLAОценок пока нет
- GPAT 16 Medicinal ChemistryДокумент19 страницGPAT 16 Medicinal ChemistryRaghava ReddyОценок пока нет
- Gpat 20Документ10 страницGpat 20GANESH KUMAR JELLAОценок пока нет
- In Vitro in Vivo Correlation 4Документ31 страницаIn Vitro in Vivo Correlation 4GANESH KUMAR JELLAОценок пока нет
- Good Laboratory PracticesДокумент39 страницGood Laboratory PracticesGANESH KUMAR JELLA100% (2)
- Liposome Drug Delivery SystemДокумент28 страницLiposome Drug Delivery SystemGANESH KUMAR JELLA100% (1)
- Gpat 18Документ25 страницGpat 18GANESH KUMAR JELLA50% (2)
- Gpat 21Документ9 страницGpat 21GANESH KUMAR JELLAОценок пока нет
- Gpat 17Документ17 страницGpat 17GANESH KUMAR JELLA0% (1)
- Gpat Model Test 1Документ21 страницаGpat Model Test 1GANESH KUMAR JELLAОценок пока нет
- Gpat Grand TestДокумент12 страницGpat Grand TestGANESH KUMAR JELLA100% (2)
- GPAT 14 P'cognosyДокумент18 страницGPAT 14 P'cognosyGANESH KUMAR JELLA86% (7)
- Gpat 9Документ15 страницGpat 9GANESH KUMAR JELLAОценок пока нет
- GPAT 13 P'ceuticsДокумент29 страницGPAT 13 P'ceuticsGANESH KUMAR JELLAОценок пока нет






















































![Basic Pharmacology And Drug Calculations [Practice Questions And Answers]](https://imgv2-2-f.scribdassets.com/img/word_document/475660044/149x198/2c7fc45015/1691161640?v=1)

























