Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- BRAND AWARENESS Proposal DocumentДокумент11 страницBRAND AWARENESS Proposal DocumentBuchi MadukaОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- TW BT 01 - Barstock Threaded Type Thermowell (Straight) : TWBT - 01Документ3 страницыTW BT 01 - Barstock Threaded Type Thermowell (Straight) : TWBT - 01Anonymous edvYngОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Acampamento 2010Документ47 страницAcampamento 2010Salete MendezОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- BECIL Registration Portal: How To ApplyДокумент2 страницыBECIL Registration Portal: How To ApplySoul BeatsОценок пока нет
- III.A.1. University of Hawaii at Manoa Cancer Center Report and Business PlanДокумент35 страницIII.A.1. University of Hawaii at Manoa Cancer Center Report and Business Planurindo mars29Оценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Geometry and IntuitionДокумент9 страницGeometry and IntuitionHollyОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Dialog+ SW9xx - SM - Chapter 7 - 2-2013 - EN - Rinsing Bridge Version 5Документ1 страницаDialog+ SW9xx - SM - Chapter 7 - 2-2013 - EN - Rinsing Bridge Version 5Al ImranОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Schneider Contactors DatasheetДокумент130 страницSchneider Contactors DatasheetVishal JainОценок пока нет
- IPM GuidelinesДокумент6 страницIPM GuidelinesHittesh SolankiОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- LG Sigma+EscalatorДокумент4 страницыLG Sigma+Escalator강민호Оценок пока нет
- N2 V Operare ManualДокумент370 страницN2 V Operare Manualramiro0001Оценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Digital SLR AstrophotographyДокумент366 страницDigital SLR AstrophotographyPier Paolo GiacomoniОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Oracle SOA Suite 11g:buildДокумент372 страницыOracle SOA Suite 11g:buildMohsen Tavakkoli100% (1)
- Mule 4 Error Handling DemystifiedДокумент8 страницMule 4 Error Handling DemystifiedNicolas boulangerОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Tetra IntroductionДокумент65 страницTetra Introductionuniversidaddistrital100% (2)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Fmicb 10 02876Документ11 страницFmicb 10 02876Angeles SuarezОценок пока нет
- Public Access - The GauntletДокумент1 страницаPublic Access - The GauntletTesting0% (2)
- Pest of Field Crops and Management PracticalДокумент44 страницыPest of Field Crops and Management PracticalNirmala RameshОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Optimal Dispatch of Generation: Prepared To Dr. Emaad SedeekДокумент7 страницOptimal Dispatch of Generation: Prepared To Dr. Emaad SedeekAhmedRaafatОценок пока нет
- Session4 Automotive Front End DesignДокумент76 страницSession4 Automotive Front End DesignShivprasad SavadattiОценок пока нет
- Building A Pentesting Lab For Wireless Networks - Sample ChapterДокумент29 страницBuilding A Pentesting Lab For Wireless Networks - Sample ChapterPackt PublishingОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Planning EngineerДокумент1 страницаPlanning EngineerChijioke ObiОценок пока нет
- Agile ModelingДокумент15 страницAgile Modelingprasad19845Оценок пока нет
- Nutrition Great Foods For Getting Vitamins A To K in Your DietДокумент1 страницаNutrition Great Foods For Getting Vitamins A To K in Your DietDhruv DuaОценок пока нет
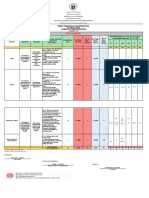
- Revised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10Документ6 страницRevised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10May Ann GuintoОценок пока нет
- Electric Vehicles PresentationДокумент10 страницElectric Vehicles PresentationVIBHU CHANDRANSH BHANOT100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Buss40004 - Balance of PowerДокумент3 страницыBuss40004 - Balance of PowerVishwa NirmalaОценок пока нет
- Better Photography - April 2018 PDFДокумент100 страницBetter Photography - April 2018 PDFPeter100% (1)
- Historical Exchange Rates - OANDA AUD-MYRДокумент1 страницаHistorical Exchange Rates - OANDA AUD-MYRML MLОценок пока нет