Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Prolapso de Cordón 1Документ10 страницProlapso de Cordón 1Jhonatan MendozaОценок пока нет
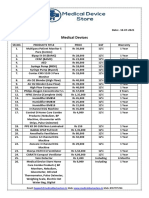
- Medical Device Store Products CatalogueДокумент3 страницыMedical Device Store Products CatalogueWasim KhatibОценок пока нет
- Provincial Drug ScheduleДокумент16 страницProvincial Drug ScheduleSamMansuriОценок пока нет
- Eligibility Criteria For (Membership Examinations) MCPSДокумент1 страницаEligibility Criteria For (Membership Examinations) MCPSmegh dutОценок пока нет
- Standard Operating Procedures For Pharmaceutical Care Delivery in Health FacilitiesДокумент7 страницStandard Operating Procedures For Pharmaceutical Care Delivery in Health FacilitiesNhu0% (1)
- Radiology MCQSДокумент23 страницыRadiology MCQSHabib Mughal67% (3)
- Breast Cancer Atlas of Clinical OncologyДокумент300 страницBreast Cancer Atlas of Clinical OncologyQueenIchma ChualunaeonelophОценок пока нет
- Screw Retained Implant LevelДокумент4 страницыScrew Retained Implant LevelorthodontistinthemakingОценок пока нет
- MCPS Family MedicineДокумент34 страницыMCPS Family MedicineWaleedAhmad100% (2)
- CHAP 21 - Immediate Loading of Dental Implants PDFДокумент15 страницCHAP 21 - Immediate Loading of Dental Implants PDFYassin SalahОценок пока нет
- Yoga and Pranayama During High-Risk PregnancyДокумент7 страницYoga and Pranayama During High-Risk PregnancyAdvanced Research PublicationsОценок пока нет
- PSDIRFДокумент3 страницыPSDIRFRandy FauskeОценок пока нет
- CHED Journal IncentiveДокумент17 страницCHED Journal IncentiveDannie PeñaОценок пока нет
- Medical Certificate - 2023 - Page 1 All AthletesДокумент2 страницыMedical Certificate - 2023 - Page 1 All AthletesAudrie Faye TabaqueОценок пока нет
- Alraqi Medical Supply Company ProfileДокумент4 страницыAlraqi Medical Supply Company ProfileKaitlyn LewisОценок пока нет
- Gowri S Reasearch ProposalДокумент12 страницGowri S Reasearch ProposalzzzzОценок пока нет
- Acute Pain NCPДокумент2 страницыAcute Pain NCPfaye-pamatmat-257080% (5)
- Amal Bhattacharya Resume - Medical PractitionerДокумент1 страницаAmal Bhattacharya Resume - Medical PractitionerSrujana MОценок пока нет
- Reproductive System Answer KeyДокумент7 страницReproductive System Answer Keyapi-209542414Оценок пока нет
- Microsoft Power Point - Tidal Therapy Approved 11-11-09Документ39 страницMicrosoft Power Point - Tidal Therapy Approved 11-11-09kamsechlerОценок пока нет
- Sme Package Summary of Benefits (2305843009215646953)Документ7 страницSme Package Summary of Benefits (2305843009215646953)RIVERA - SARVIDA CONSTRUCTION INC.Оценок пока нет
- Code Team Training and Assessment Best Practices From The Floor UCM - 486059Документ34 страницыCode Team Training and Assessment Best Practices From The Floor UCM - 486059JoaoОценок пока нет
- Laparoscopic Instruments-AlcabedosДокумент8 страницLaparoscopic Instruments-AlcabedosHydie Mae AlcabedosОценок пока нет
- Deterioration in Pregnant or Recently Delivered Women MeowsДокумент17 страницDeterioration in Pregnant or Recently Delivered Women MeowsYudi WiraОценок пока нет
- Fi Bro AdenomaДокумент2 страницыFi Bro AdenomafebrianaayupОценок пока нет
- Biography Report Template UPS6002AДокумент4 страницыBiography Report Template UPS6002AAkanksha KulkarniОценок пока нет
- Naima - Magnitude and Risk Factors For Puerperal Sepsis at The Pumwani Maternity Hospital.Документ61 страницаNaima - Magnitude and Risk Factors For Puerperal Sepsis at The Pumwani Maternity Hospital.PaulОценок пока нет
- Nlex 1Документ4 страницыNlex 1Aileen AlphaОценок пока нет
- A Study On Internal Fixation of Bimalleolar Ankle FracturesДокумент4 страницыA Study On Internal Fixation of Bimalleolar Ankle FracturesIOSRjournalОценок пока нет