Вам также может понравиться
- Hirsutism: Diagnosis and TreatmentДокумент6 страницHirsutism: Diagnosis and TreatmentAnonymous ysrxggk21cОценок пока нет
- Lourence M. Patagoc Block 1 SGD Group 1 Module 2 GYNE Case Hirsutism and VirilizationДокумент48 страницLourence M. Patagoc Block 1 SGD Group 1 Module 2 GYNE Case Hirsutism and VirilizationFernando AnibanОценок пока нет
- Amenorrhea and SpaniomenorrheasДокумент59 страницAmenorrhea and SpaniomenorrheasIdiAmadouОценок пока нет
- Evaluacion HirsutismoДокумент8 страницEvaluacion HirsutismoAli ChongОценок пока нет
- Hirsutism: Clinical PracticeДокумент11 страницHirsutism: Clinical PracticeAnonymous kltUTaОценок пока нет
- PCOS-Epidemiology: Age Which Approximately 4 Million IndividualsДокумент66 страницPCOS-Epidemiology: Age Which Approximately 4 Million IndividualsAseel wael alshareefОценок пока нет
- Hirsutism and HomoeopathyДокумент9 страницHirsutism and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Obstetrics and Gynecology Sixth Edition Obstetrics and Gynecology Beckman Chapter 36Документ8 страницObstetrics and Gynecology Sixth Edition Obstetrics and Gynecology Beckman Chapter 363hondoОценок пока нет
- Pediatric Endocrinology Review MCQS: Part - 4Документ33 страницыPediatric Endocrinology Review MCQS: Part - 4Reem 10Оценок пока нет
- AmenorrheaДокумент51 страницаAmenorrheaAyalewОценок пока нет
- 26 PcosДокумент66 страниц26 PcosdenekeОценок пока нет
- Pituitary DisorderДокумент34 страницыPituitary DisorderSoniya ShivanshОценок пока нет
- Polycystic Ovarian SyndromeДокумент11 страницPolycystic Ovarian Syndromezianab aliОценок пока нет
- Presentation 2Документ43 страницыPresentation 2talaarar695Оценок пока нет
- Work Up of Gynecomastia (Slides)Документ22 страницыWork Up of Gynecomastia (Slides)rajan kumar67% (3)
- PCOSДокумент38 страницPCOSJitendra Chaudhary100% (1)
- W4-24 Amenorrhea, Hyperandogenism - LectureДокумент73 страницыW4-24 Amenorrhea, Hyperandogenism - LectureVivek ChourhaОценок пока нет
- Secamenhyper 120208102817 Phpapp02Документ31 страницаSecamenhyper 120208102817 Phpapp02Mohan DassОценок пока нет
- Jurnal PCOSДокумент39 страницJurnal PCOSGian Alodia RisamasuОценок пока нет
- AmenorrheaДокумент70 страницAmenorrheagimОценок пока нет
- Endocrine PathologyДокумент60 страницEndocrine PathologySingitan SiyoumОценок пока нет
- Testicular Feminization Syndrome: SGD B-3Документ29 страницTesticular Feminization Syndrome: SGD B-3Jessica LinОценок пока нет
- Physiotherapy in PCOSДокумент54 страницыPhysiotherapy in PCOSAkshaya Nayak100% (3)
- Female Infertility: DR Jaqueline Sudiman, PHDДокумент21 страницаFemale Infertility: DR Jaqueline Sudiman, PHDGlorio Absalom PuaОценок пока нет
- HYPERANDROGENISMДокумент73 страницыHYPERANDROGENISMmarc_caronan100% (1)
- Acromegaly: Atwebembere Raymond 214-083011-07132 Dr. Ssebuliba MosesДокумент32 страницыAcromegaly: Atwebembere Raymond 214-083011-07132 Dr. Ssebuliba MosesNinaОценок пока нет
- Nursing Care For HipopituitarismeДокумент10 страницNursing Care For Hipopituitarismevita marta100% (1)
- Lecture 3 Thyroid, Parathyroid and Adrenal GlandДокумент74 страницыLecture 3 Thyroid, Parathyroid and Adrenal GlandMuhammad ShayanОценок пока нет
- Amenorrhea WilliamsДокумент26 страницAmenorrhea WilliamsGregorius Juan GunawanОценок пока нет
- Amenorrhea SGDДокумент44 страницыAmenorrhea SGDMichelle Lariosa ChangОценок пока нет
- Female Infertility: DR Jaqueline Sudiman, PHDДокумент21 страницаFemale Infertility: DR Jaqueline Sudiman, PHDJuli FionaОценок пока нет
- Hyperestrinism, Klinefelter and Super MalesДокумент39 страницHyperestrinism, Klinefelter and Super MalesGerald John Paz100% (1)
- Azdihar Lec 9 InfertilityДокумент37 страницAzdihar Lec 9 Infertilityalmastar officeОценок пока нет
- Polycystic Ovarian SyndromeДокумент20 страницPolycystic Ovarian SyndromeMuhammad khairul afizal RohimОценок пока нет
- Polycystic Ovarian Syndrome (PCOS)Документ119 страницPolycystic Ovarian Syndrome (PCOS)Jasani JayrajОценок пока нет
- Evaluation of Infertile CoupleДокумент70 страницEvaluation of Infertile CoupleNdenwaneku OkuwaОценок пока нет
- Subclinical Thyroid DiseaseДокумент50 страницSubclinical Thyroid Diseaseกรคุง ภิญโญพจนารถОценок пока нет
- HyperpituitarismДокумент25 страницHyperpituitarismBheru Lal0% (1)
- Androgen Excess and PCOSДокумент50 страницAndrogen Excess and PCOSRica MarquezОценок пока нет
- Amenorrhea: DR - Raveendra MVДокумент23 страницыAmenorrhea: DR - Raveendra MVRaveendra M.vОценок пока нет
- Disorders of Growth Hormone: Practical Endocrinology Wendy Blount, DVMДокумент47 страницDisorders of Growth Hormone: Practical Endocrinology Wendy Blount, DVMAbdallah AlasalОценок пока нет
- Skin Abnormality and Hairloss: The Reproductive Endocrinological ViewpointДокумент6 страницSkin Abnormality and Hairloss: The Reproductive Endocrinological ViewpointZenithОценок пока нет
- PCOS-GYN CaseДокумент17 страницPCOS-GYN CaseLaya ChararaОценок пока нет
- Cushing's Syndrome: Hyperadrenocorticism Is An EndocrineДокумент17 страницCushing's Syndrome: Hyperadrenocorticism Is An EndocrineFernando Junior Parra UchasaraОценок пока нет
- Physiology of MenopauseДокумент35 страницPhysiology of Menopauseamjad100% (1)
- Endocrine DisodersДокумент330 страницEndocrine Disodersbrianmuthomi851Оценок пока нет
- Disorders of The Endocrine SystemДокумент84 страницыDisorders of The Endocrine Systemcy lifeОценок пока нет
- Week 1 - Women Health DisordersДокумент41 страницаWeek 1 - Women Health Disordersmemoona kaleemОценок пока нет
- PCOS DR BasimaДокумент18 страницPCOS DR BasimaA.H.AОценок пока нет
- EndoДокумент252 страницыEndoyuuki konnoОценок пока нет
- HypothyroidismДокумент59 страницHypothyroidismAmir Mahmoud100% (1)
- MEETING 6 AmenorrheaДокумент41 страницаMEETING 6 AmenorrheaNader KhouryОценок пока нет
- Pediatric Endocrinology Review MCQsДокумент104 страницыPediatric Endocrinology Review MCQsTirou100% (1)
- Approach To Endocrinology Disorders: Kurniyanto Department of Internal Medicine FK UkiДокумент36 страницApproach To Endocrinology Disorders: Kurniyanto Department of Internal Medicine FK UkiDaud ParluhutanОценок пока нет
- Vaginal Atrophy ElghanyДокумент74 страницыVaginal Atrophy Elghanykhadzx100% (3)
- HyperpitutrismДокумент41 страницаHyperpitutrismmuhammad kazimОценок пока нет
- Management of MenopauseДокумент55 страницManagement of MenopauseMohmmed Al ShamasinОценок пока нет
- Polycystic Ovarian SyndromeДокумент47 страницPolycystic Ovarian SyndromeAnonymous HgX3mN1o100% (1)
- HormonesДокумент23 страницыHormonesKU ExergonicОценок пока нет
- Kasus Istimewa - Amenorrhea PrimerДокумент45 страницKasus Istimewa - Amenorrhea PrimerMuhammad SukriОценок пока нет
- Normal Menstrual CycleДокумент28 страницNormal Menstrual CycleCristóbal ConchaОценок пока нет
- Endo Lect-Ant Pituitary GlandДокумент18 страницEndo Lect-Ant Pituitary GlanddoctorrfarrukhОценок пока нет
- BHSAgriculture - The Role of Hormones in The Regulation of Animal Reproduction and BehaviourДокумент2 страницыBHSAgriculture - The Role of Hormones in The Regulation of Animal Reproduction and BehaviourzuhaibОценок пока нет
- SAB HLTAAP001 Recognise Healthy Body SystemsДокумент67 страницSAB HLTAAP001 Recognise Healthy Body SystemsBbas T.95% (20)
- Thyroid Function Ordering AlgorithmДокумент1 страницаThyroid Function Ordering AlgorithmMVKDSP RaoОценок пока нет
- Chronic Kidney Disease: A. Pathophysiology A. Schematic DiagramДокумент3 страницыChronic Kidney Disease: A. Pathophysiology A. Schematic DiagramDaniel GeduquioОценок пока нет
- Investigatii ParacliniceДокумент3 страницыInvestigatii ParaclinicebobcristibobОценок пока нет
- Group 4 - Introduction To Pathology - M1 ActivityДокумент2 страницыGroup 4 - Introduction To Pathology - M1 ActivityJim IsmaelОценок пока нет
- Unit 7 Diabetes Student ResourcesДокумент7 страницUnit 7 Diabetes Student ResourcesScribdОценок пока нет
- Thyroid Storm: Karthik Balachandran Karthik2k2Документ52 страницыThyroid Storm: Karthik Balachandran Karthik2k2Dr Karthik Balachandran, EndocrinologyОценок пока нет
- Chap 31 HWДокумент12 страницChap 31 HWizabelaОценок пока нет
- Concept Map of DMДокумент2 страницыConcept Map of DMLeslie Marie Rendon100% (9)
- Multiple-Choice QuizДокумент6 страницMultiple-Choice QuizHUAWEI HUAWEI100% (1)
- Pheochromocytoma-A Case PresentationДокумент14 страницPheochromocytoma-A Case Presentationdidu91Оценок пока нет
- Chapter 15- Jnu Cellular Signaling - 複本Документ49 страницChapter 15- Jnu Cellular Signaling - 複本Wai Kwong ChiuОценок пока нет
- Unit IV Lecture NotesДокумент9 страницUnit IV Lecture NotesSteve SullivanОценок пока нет
- Gigantism PresentationДокумент24 страницыGigantism PresentationYaseen MohmandОценок пока нет
- Pathogenesis of Type 2 Diabetes Mellitus (Dr. Dr. Pugud Samodro, SP - PD, KEMD, FINASIM)Документ33 страницыPathogenesis of Type 2 Diabetes Mellitus (Dr. Dr. Pugud Samodro, SP - PD, KEMD, FINASIM)Yohan Parulian SinagaОценок пока нет
- Dr. Syafrizal Syafei Basic Principle and Administration of Hormonal and Intgreated Therapy in CancerДокумент28 страницDr. Syafrizal Syafei Basic Principle and Administration of Hormonal and Intgreated Therapy in CancerWilliamRayCassidyОценок пока нет
- Diagnostic Test For Endocrine DisordersДокумент15 страницDiagnostic Test For Endocrine DisordersRichard Deo R. Alave100% (1)
- Readingtest 3Документ19 страницReadingtest 3SevvalОценок пока нет
- Reaction Paper Rizal PlumaДокумент33 страницыReaction Paper Rizal PlumaJazzd Sy Gregorio0% (1)
- Laboratory Diagnostics of (Selected) Endocrine DisordersДокумент48 страницLaboratory Diagnostics of (Selected) Endocrine DisordersPaulina PaskeviciuteОценок пока нет
- Management of Hyperglycemia in Hospitalized Adult Patients in Non-Critical Care Settings: An Endocrine Society Clinical Practice GuidelineДокумент34 страницыManagement of Hyperglycemia in Hospitalized Adult Patients in Non-Critical Care Settings: An Endocrine Society Clinical Practice Guidelineakash kondapalliОценок пока нет
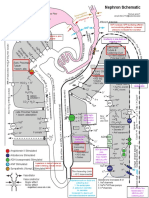
- NephronMap Copy2Документ1 страницаNephronMap Copy2Anonymous KxwaMDhAОценок пока нет
- Maternity Nursing ReviewДокумент52 страницыMaternity Nursing ReviewDragan Petrovic100% (1)
- Compendiumofanimalreproduction 160518055221Документ506 страницCompendiumofanimalreproduction 160518055221ابراهيم القويعىОценок пока нет
- Prediabetes - OKE - IDI LMGNДокумент48 страницPrediabetes - OKE - IDI LMGNruthmindosiahaanОценок пока нет