Вам также может понравиться
- Bacterial Skin Infections GuideДокумент41 страницаBacterial Skin Infections GuideUmmi Rinandari100% (1)
- Fungal Infections of the Skin, Hair and NailsДокумент120 страницFungal Infections of the Skin, Hair and NailsmissirenaОценок пока нет
- Skin Infections and InfestationsДокумент37 страницSkin Infections and InfestationsAremu OlatayoОценок пока нет
- Superficial and Cutaneous MycosesДокумент34 страницыSuperficial and Cutaneous MycosesPrincewill Seiyefa100% (1)
- Anthropophilic Geophilic Zoophilic Source: No. of Conidia (Culture Medium) Tissue Reaction ExamplesДокумент6 страницAnthropophilic Geophilic Zoophilic Source: No. of Conidia (Culture Medium) Tissue Reaction ExamplesAaron James RuedasОценок пока нет
- Systemic Lupus ErythematosusДокумент46 страницSystemic Lupus ErythematosuspriscillaОценок пока нет
- Bacterial Infections of SkinДокумент72 страницыBacterial Infections of SkinSiddharth DashОценок пока нет
- Fungal InfectionsДокумент42 страницыFungal InfectionsleenaloveuОценок пока нет
- SyphilisДокумент3 страницыSyphilisstaci_lutchman100% (2)
- CandidiasisДокумент27 страницCandidiasisfarmasi_hmОценок пока нет
- Vector-Borne Diseases in the Philippines: An OverviewДокумент42 страницыVector-Borne Diseases in the Philippines: An OverviewCyra Oynang100% (1)
- Superficial and Cutaneous MycosesДокумент4 страницыSuperficial and Cutaneous Mycosessarguss14Оценок пока нет
- Rabies Virus, Disease, and PreventionДокумент25 страницRabies Virus, Disease, and PreventionAdindapauliaОценок пока нет
- Gas Gangrene.Документ24 страницыGas Gangrene.Jared GreenОценок пока нет
- PsoriasisДокумент32 страницыPsoriasisChirag VijayvargiyaОценок пока нет
- Malaria Parasites and Their Life CyclesДокумент66 страницMalaria Parasites and Their Life CyclesDaxОценок пока нет
- Japanese Encephalitis by RobelДокумент2 страницыJapanese Encephalitis by RobelRobel_Saoi_2309Оценок пока нет
- Intraventricular Hemorrhage (IVH) : Intensive Care Nursery House Staff ManualДокумент3 страницыIntraventricular Hemorrhage (IVH) : Intensive Care Nursery House Staff Manualjimzz44Оценок пока нет
- Deepshikha Chhetri Msc. FSNДокумент50 страницDeepshikha Chhetri Msc. FSNDaiane SantanaОценок пока нет
- Syphilis: Etiology, Pathogenesis, Transmission, Stages, Manifestations and TreatmentДокумент39 страницSyphilis: Etiology, Pathogenesis, Transmission, Stages, Manifestations and TreatmentEINSTEIN2D100% (1)
- Fungal Infections of HumansДокумент22 страницыFungal Infections of HumansJhara100% (2)
- Krizia Joy Borromeo-Galve, MD: Bulacan Medical Center, Department of PediatricsДокумент84 страницыKrizia Joy Borromeo-Galve, MD: Bulacan Medical Center, Department of PediatricsTara Oliveros Dela CruzОценок пока нет
- Mycoses: Mallare - Morales - QuibalДокумент67 страницMycoses: Mallare - Morales - QuibalBianca MoralesОценок пока нет
- SyphilisДокумент89 страницSyphilisAnuZ13thОценок пока нет
- Neisseria gonorrhoeae (GonococcusДокумент28 страницNeisseria gonorrhoeae (GonococcusRoni Ananda Perwira HarahapОценок пока нет
- National TB ProgramДокумент54 страницыNational TB Programarlian malihanОценок пока нет
- Tonsillitis: Anatomy, Physiology, Diagnosis and ManagementДокумент19 страницTonsillitis: Anatomy, Physiology, Diagnosis and ManagementDanica Camille PanlilioОценок пока нет
- TetanusДокумент26 страницTetanusCharlize Andrea DiestaОценок пока нет
- Filaria PPT - ClassДокумент59 страницFilaria PPT - ClassGauravMeratwal100% (2)
- Lesions PPT NewДокумент37 страницLesions PPT NewDeb SharmaОценок пока нет
- Basics Mycology SQ 2009-10Документ3 страницыBasics Mycology SQ 2009-10fateh2100% (1)
- SANDRA, Apollo OBG Minor Disorders in Neonates PPT - SECTION BДокумент15 страницSANDRA, Apollo OBG Minor Disorders in Neonates PPT - SECTION Bsandra0% (1)
- Brucellosis 2Документ70 страницBrucellosis 2Zara IftikharОценок пока нет
- Gram Negative SpirochetesДокумент50 страницGram Negative SpirochetesYeshiwas FelekeОценок пока нет
- Hypersensitivity Reactions BasicsДокумент101 страницаHypersensitivity Reactions Basicstummalapalli venkateswara rao100% (1)
- Cholera: Dr. Priyanka SachdevaДокумент71 страницаCholera: Dr. Priyanka Sachdevapriyanka100% (1)
- What is Enteric FeverДокумент22 страницыWhat is Enteric FeverRuchika SharmaОценок пока нет
- General Characteristics of VirusesДокумент3 страницыGeneral Characteristics of VirusesLyraski BalawisОценок пока нет
- Hypersensitivity Types and MechanismsДокумент37 страницHypersensitivity Types and MechanismskiguzonОценок пока нет
- Tuberculous Meningitis Diagnosis, Treatment and Impact of HIVДокумент34 страницыTuberculous Meningitis Diagnosis, Treatment and Impact of HIVLuvi PujiОценок пока нет
- Understanding Chlamydiae InfectionsДокумент32 страницыUnderstanding Chlamydiae InfectionsNaing Lin SoeОценок пока нет
- MENINGITISДокумент44 страницыMENINGITIStummalapalli venkateswara rao100% (5)
- Deep Fungal InfectionДокумент39 страницDeep Fungal InfectionFahmi Nur AL-HidayatОценок пока нет
- Pox VirusesДокумент11 страницPox VirusesSarah PavuОценок пока нет
- AIDS Teaching ModuleДокумент122 страницыAIDS Teaching Moduletummalapalli venkateswara raoОценок пока нет
- MHC Molecules and T Cell ReceptorsДокумент39 страницMHC Molecules and T Cell Receptors16_dev5038100% (1)
- Infectious DiseasesДокумент13 страницInfectious DiseasesRavneetKalkatОценок пока нет
- Bacterial Skin Infections GuideДокумент138 страницBacterial Skin Infections GuideArwi WijayaОценок пока нет
- Prevalence of Teenage Pregnancy Among Pregnant Mothers Presenting at Hoima Regional Referral Hospital During The Covid-19 Pandemic (2020 To 2021)Документ8 страницPrevalence of Teenage Pregnancy Among Pregnant Mothers Presenting at Hoima Regional Referral Hospital During The Covid-19 Pandemic (2020 To 2021)KIU PUBLICATION AND EXTENSIONОценок пока нет
- Typhoid FeverДокумент27 страницTyphoid FeverApril Mergelle Lapuz100% (1)
- Representative Questions on Fungal Lectures and LabsДокумент8 страницRepresentative Questions on Fungal Lectures and LabsYousefM.R.AlmassriОценок пока нет
- Haemophilus SPPДокумент109 страницHaemophilus SPPJamie CañebaОценок пока нет
- Intestinal Helminthiasis and Filariasis - SGTДокумент73 страницыIntestinal Helminthiasis and Filariasis - SGTLemathaОценок пока нет
- NeisseriaДокумент32 страницыNeisseriaKeshant SamarooОценок пока нет
- Hypersensitivity: by Yundzir FurqanДокумент18 страницHypersensitivity: by Yundzir FurqanFuЯqanFriesОценок пока нет
- Lecture 1 - InfluenzaДокумент67 страницLecture 1 - InfluenzaShaimaa AbdulkadirОценок пока нет
- MeaslesДокумент23 страницыMeaslesadwait marhattaОценок пока нет
- Solid Waste Management For Hospitals: Presented By: Faisal V A MT15CTM004Документ46 страницSolid Waste Management For Hospitals: Presented By: Faisal V A MT15CTM004vnitceОценок пока нет
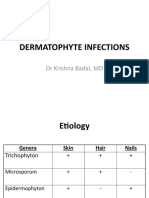
- Dermatophyte InfectionsДокумент41 страницаDermatophyte Infectionsshoaib khanОценок пока нет
- K7 Jamur Superficial 2020Документ51 страницаK7 Jamur Superficial 2020Jimmy Fran IIОценок пока нет
- Immunity To InfectionsДокумент19 страницImmunity To Infectionsapi-3699361100% (1)
- Para1 FemaleДокумент4 страницыPara1 Femaleapi-3699361Оценок пока нет
- Introduction Models and Methods of Understanding Human2Документ26 страницIntroduction Models and Methods of Understanding Human2api-3699361100% (1)
- As 1Документ28 страницAs 1api-3699361Оценок пока нет
- Testing Hypothesis 2Документ16 страницTesting Hypothesis 2api-3699361Оценок пока нет
- IntroductionДокумент19 страницIntroductionapi-3699361Оценок пока нет
- Antigen Antibody and T InteractionsДокумент16 страницAntigen Antibody and T Interactionsapi-3699361Оценок пока нет
- Cells of The Immune SystemДокумент21 страницаCells of The Immune Systemapi-3699361Оценок пока нет
- Antigens and HLAДокумент16 страницAntigens and HLAapi-3699361Оценок пока нет
- Innate ImmunityДокумент12 страницInnate Immunityapi-3699361Оценок пока нет
- Acquired ImmunityДокумент18 страницAcquired Immunityapi-3699361Оценок пока нет
- EstimationДокумент7 страницEstimationapi-3699361Оценок пока нет
- AntibodiesДокумент29 страницAntibodiesapi-3699361Оценок пока нет
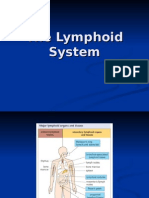
- Lymphoid System MedicineДокумент21 страницаLymphoid System Medicineapi-3699361Оценок пока нет
- Induction of Immune ResponsesДокумент19 страницInduction of Immune Responsesapi-3699361Оценок пока нет
- CytokinesДокумент10 страницCytokinesapi-3699361Оценок пока нет
- Case 2Документ22 страницыCase 2api-3699361Оценок пока нет
- Parsites ScheduleДокумент2 страницыParsites Scheduleapi-3699361Оценок пока нет
- Motor System Spinal Cord2Документ45 страницMotor System Spinal Cord2api-3699361Оценок пока нет
- Reflexes LabДокумент13 страницReflexes Labapi-3699361Оценок пока нет
- Salmonell and Shigella Lab-13Документ10 страницSalmonell and Shigella Lab-13api-3699361Оценок пока нет
- Stool Culture Lab 150Документ10 страницStool Culture Lab 150api-3699361Оценок пока нет
- Mycobacterium Tuberculosis Lab14Документ11 страницMycobacterium Tuberculosis Lab14api-3699361Оценок пока нет
- Motor System Cerebral CortexДокумент28 страницMotor System Cerebral Cortexapi-3699361Оценок пока нет
- Approaches To PsychotherapyДокумент4 страницыApproaches To PsychotherapyHassan.shehri100% (7)
- Motor System 1Документ30 страницMotor System 1api-36993610% (1)
- Developmental PsychologyДокумент9 страницDevelopmental PsychologyHassan.shehri100% (2)
- Learn MedДокумент6 страницLearn Medapi-3699361Оценок пока нет
- Human MemoryДокумент5 страницHuman Memoryapi-3699361Оценок пока нет
- Models of Understanding Human BehaviourДокумент3 страницыModels of Understanding Human BehaviourHassan.shehri94% (18)
- Streptococcus PneumoniaДокумент2 страницыStreptococcus PneumoniaElishah CaprichoОценок пока нет
- Moraxella: The Bacteria That Causes Ear Infections and MoreДокумент20 страницMoraxella: The Bacteria That Causes Ear Infections and Moreshinwar benyamenОценок пока нет
- Minncare Against Specific MicroДокумент1 страницаMinncare Against Specific MicroRidwan ArifandiОценок пока нет
- Unknown Lab Report 13Документ20 страницUnknown Lab Report 13jordan holstОценок пока нет
- Microbiology Practice Test IIIДокумент14 страницMicrobiology Practice Test IIISidharta ChatterjeeОценок пока нет
- Ziehl Neelsen Staining (Pewarnaan Tahan Asam)Документ4 страницыZiehl Neelsen Staining (Pewarnaan Tahan Asam)SALSABILA AMANIAОценок пока нет
- Andrews Diseases of The Skin Clinical Dermatology, 12th Ed - James, Berger, Elston, & Neuhaus - LTДокумент2 страницыAndrews Diseases of The Skin Clinical Dermatology, 12th Ed - James, Berger, Elston, & Neuhaus - LTsyed rokunujjamanОценок пока нет
- Ppra Snars I Dr. DewiДокумент93 страницыPpra Snars I Dr. DewiNilam atika sariОценок пока нет
- 7708 21480 1 PB PDFДокумент8 страниц7708 21480 1 PB PDFAnnisa ZaharaОценок пока нет
- SB 3 Flu VaccineДокумент2 страницыSB 3 Flu VaccineBIANNE KATRINA GASAGASОценок пока нет
- CL7 Urinary Tract Infection 20192020-20191212060056Документ50 страницCL7 Urinary Tract Infection 20192020-20191212060056Nur Ain IzzatiОценок пока нет
- Halophilic and Halotolerant MicrobesДокумент5 страницHalophilic and Halotolerant MicrobesAdri De UdokОценок пока нет
- Blood Culture Collection and InterpretationДокумент10 страницBlood Culture Collection and InterpretationMaria Chacón CarbajalОценок пока нет
- M LepraeДокумент10 страницM Lepraebmc microОценок пока нет
- Human Parasitology Slides IntroДокумент53 страницыHuman Parasitology Slides Introslyfoxkitty100% (1)
- All About Rabies Health ScienceДокумент28 страницAll About Rabies Health SciencetototoОценок пока нет
- Instructions To Disembarking CrewДокумент8 страницInstructions To Disembarking CrewNelfa Dela CruzОценок пока нет
- Sarcocystis SpeciesДокумент16 страницSarcocystis SpeciesChristianОценок пока нет
- Presentor: Instructor: Firm:: Dr. Posiano Phiri DR Shankanga PinkДокумент10 страницPresentor: Instructor: Firm:: Dr. Posiano Phiri DR Shankanga PinkPeter TambweОценок пока нет
- Anaerobe of Clinical ImportanceДокумент43 страницыAnaerobe of Clinical ImportanceDayledaniel SorvetoОценок пока нет
- Worksheet 6: Special Bacterial Structures: Learning ObjectivesДокумент4 страницыWorksheet 6: Special Bacterial Structures: Learning ObjectivesRaphael KevinОценок пока нет
- 1526931608Документ229 страниц1526931608MKGUОценок пока нет
- Microbiology MCQ QuestionsДокумент4 страницыMicrobiology MCQ QuestionsNWH Adams LabОценок пока нет
- Micro Malathi Murugesan MICRONS PDFДокумент579 страницMicro Malathi Murugesan MICRONS PDFBharat G100% (2)
- Street Food Vending: A Case Study From Assam, India: Chandrama Baruah, Ruma Bhattacharyya, Pranati Das and Pranab DuttaДокумент7 страницStreet Food Vending: A Case Study From Assam, India: Chandrama Baruah, Ruma Bhattacharyya, Pranati Das and Pranab DuttaGanavi JОценок пока нет
- Antibacterial Activity of Cupric Oxide Nanoparticles Against Pathogenic BacteriaДокумент4 страницыAntibacterial Activity of Cupric Oxide Nanoparticles Against Pathogenic BacteriaNILTHON FRANCO POMA HUARINGAОценок пока нет
- Micro CardsДокумент152 страницыMicro CardsasmaОценок пока нет
- Quantitative and Qualitative Evaluation of Three CДокумент7 страницQuantitative and Qualitative Evaluation of Three COlga CobilasОценок пока нет
- Blackhead Disease: Navigation SearchДокумент8 страницBlackhead Disease: Navigation SearchSUTHANОценок пока нет
- Rabies Elephants Srilanka 1st Report CaseДокумент2 страницыRabies Elephants Srilanka 1st Report CaseSuraj_SubediОценок пока нет