Вам также может понравиться
- Dengue Fever in The PhilippinesДокумент27 страницDengue Fever in The PhilippinesDale Marie RenomeronОценок пока нет
- Crush Your Public Speaking Fears: Speak To InspireДокумент3 страницыCrush Your Public Speaking Fears: Speak To Inspiredebanikg0% (1)
- MedicationДокумент32 страницыMedicationسلطان القلحОценок пока нет
- Surgical Treatment For BREAST CANCERДокумент5 страницSurgical Treatment For BREAST CANCERJericho James TopacioОценок пока нет
- Self Directive LearningДокумент18 страницSelf Directive Learningcrystal fate valdezОценок пока нет
- Sanctification of The Heart 4th Edition by DR Michelle StrydomДокумент771 страницаSanctification of The Heart 4th Edition by DR Michelle StrydomDios Estrella67% (3)
- HTN BrochureДокумент2 страницыHTN Brochureapi-400548889Оценок пока нет
- Pathophysiology: Cardiovascular Diseases Coronary Artery Disease (CAD)Документ5 страницPathophysiology: Cardiovascular Diseases Coronary Artery Disease (CAD)Grace Bernadine H. Ramos100% (1)
- Infertility Stress DepressionДокумент2 страницыInfertility Stress DepressionLily LavenderОценок пока нет
- 24hr Fluid Balance ADULT Chart - v3Документ2 страницы24hr Fluid Balance ADULT Chart - v3anggita diah100% (1)
- Food and Water-Borne Diseases PDFДокумент51 страницаFood and Water-Borne Diseases PDFKeo De Leon100% (1)
- Central Nervous System InfectionsДокумент51 страницаCentral Nervous System Infectionsmedtech_22m100% (1)
- Hypertension Brochure PeДокумент3 страницыHypertension Brochure Peapi-348353977Оценок пока нет
- BREECH 2nijnjinijnuihiuhДокумент7 страницBREECH 2nijnjinijnuihiuhChethranОценок пока нет
- C Anticholinergic Drugs PDFДокумент53 страницыC Anticholinergic Drugs PDFHitesh karnОценок пока нет
- Seminar on Identifying High Risk PregnanciesДокумент23 страницыSeminar on Identifying High Risk PregnanciesHaripriya RadhikaОценок пока нет
- Diabetes BrochureДокумент3 страницыDiabetes Brochureapi-498987425Оценок пока нет
- Perioperative Pain ManagementДокумент6 страницPerioperative Pain ManagementAya RandallОценок пока нет
- LeprosyДокумент16 страницLeprosyPriscilla Sund Nguyen100% (2)
- Maternal & Child HealthДокумент84 страницыMaternal & Child HealthAnjum AbbasiОценок пока нет
- Introduction To Medical Ethics: Presenter: DR Purva Shoor Assistant Professor Community MedicineДокумент33 страницыIntroduction To Medical Ethics: Presenter: DR Purva Shoor Assistant Professor Community MedicineDr purva ShoorОценок пока нет
- Cerebral EdemaДокумент40 страницCerebral EdemaMithun GorreОценок пока нет
- Intestinal Polyps and PolyposisДокумент244 страницыIntestinal Polyps and PolyposisVladislav KotovОценок пока нет
- Better Than I Found It: Stories of Patient Experience and Healthcare LeadershipОт EverandBetter Than I Found It: Stories of Patient Experience and Healthcare LeadershipОценок пока нет
- Litrature & Case StudyДокумент74 страницыLitrature & Case Studynaol buloОценок пока нет
- GEA ProtocolsДокумент101 страницаGEA Protocolsffbrians100% (1)
- Review of Literature on Rabies Prevention and ControlДокумент24 страницыReview of Literature on Rabies Prevention and ControlBeah Claudette AbundoОценок пока нет
- Cohort Study DesignДокумент34 страницыCohort Study DesignErmiasОценок пока нет
- Environmental EmergenciesДокумент38 страницEnvironmental EmergenciesIshaBrijeshSharmaОценок пока нет
- 10 Signs Death Is Near: Recognizing the Natural Dying ProcessДокумент5 страниц10 Signs Death Is Near: Recognizing the Natural Dying ProcessJay SmithОценок пока нет
- Neonatal Emergencies FinalДокумент90 страницNeonatal Emergencies FinalDr Raseena VattamkandathilОценок пока нет
- AppendectomyДокумент7 страницAppendectomyJoffy MarshallОценок пока нет
- Acute Respiratory Distress SyndromeДокумент36 страницAcute Respiratory Distress Syndromedr9348345000Оценок пока нет
- Acute Respiratory Distress SyndromeДокумент36 страницAcute Respiratory Distress Syndromedr9348345000Оценок пока нет
- Hand-Foot-Mouth DiseaseДокумент28 страницHand-Foot-Mouth Diseasebrillniks100% (2)
- Become A Better You: 7 Keys To Improving Your Life Every Day Author: Joel OsteenДокумент38 страницBecome A Better You: 7 Keys To Improving Your Life Every Day Author: Joel OsteenIdowu AfeОценок пока нет
- Feline Asthma: Laura A. Nafe, DVM, MS, Dacvim (Saim)Документ5 страницFeline Asthma: Laura A. Nafe, DVM, MS, Dacvim (Saim)Miruna ChiriacОценок пока нет
- Cpm15th Dengue Fever (Doh)Документ18 страницCpm15th Dengue Fever (Doh)Marko ParungoОценок пока нет
- DengueДокумент41 страницаDengueJonathan00711100% (1)
- 4S Strategy Crucial for Dengue PreventionДокумент5 страниц4S Strategy Crucial for Dengue PreventionJulius Linsangan De GuzmanОценок пока нет
- ANTENATAL, INTRANATAL & POSTNATAL CARE GUIDEДокумент108 страницANTENATAL, INTRANATAL & POSTNATAL CARE GUIDEumesh chhotalaОценок пока нет
- Diagnosis and Treatment of Otitis Media in ChildrenДокумент19 страницDiagnosis and Treatment of Otitis Media in ChildrenreyhanrrОценок пока нет
- Mwami Schools of Nursing and Midwifery: by Baldwin Hamoonga 5 Year Nursing Student (Ru) Topic: Small For Dates BabyДокумент26 страницMwami Schools of Nursing and Midwifery: by Baldwin Hamoonga 5 Year Nursing Student (Ru) Topic: Small For Dates BabyBaldwin Hamzcorp HamoongaОценок пока нет
- Homeostasis Temperature RegulationДокумент22 страницыHomeostasis Temperature RegulationChris AllamОценок пока нет
- Community Health Nursing ManualДокумент23 страницыCommunity Health Nursing ManualNurjanna AdjilulОценок пока нет
- Individual Assignment 1 Petco Case StudyДокумент6 страницIndividual Assignment 1 Petco Case StudyNusrat PromeОценок пока нет
- Biochem Mixed QuestionsДокумент220 страницBiochem Mixed QuestionsAnonymous xk7cBdFОценок пока нет
- Discharge Planning PathwayДокумент26 страницDischarge Planning PathwayEndah SetyawatiОценок пока нет
- MumpsДокумент7 страницMumpsKristine DolatreОценок пока нет
- About Rubella: VaccineДокумент5 страницAbout Rubella: VaccinejudssalangsangОценок пока нет
- Group 5 13B: End Stage Renal Failure Secondary To Diabetes NephropathyДокумент68 страницGroup 5 13B: End Stage Renal Failure Secondary To Diabetes NephropathyJinski007100% (1)
- F0018 CCTC DialysisДокумент4 страницыF0018 CCTC Dialysiszenagit123456Оценок пока нет
- Leadership and ManagementДокумент70 страницLeadership and ManagementElaisa Mae Delos Santos100% (3)
- National Control of Dirrheal Diseases (CDD) Program ObjectivesДокумент6 страницNational Control of Dirrheal Diseases (CDD) Program ObjectivesJoy FucananОценок пока нет
- CGAtoolДокумент17 страницCGAtoolGlory Anne Joy WillyОценок пока нет
- Flip Chart: Integrated Management of Childhood IllnessДокумент24 страницыFlip Chart: Integrated Management of Childhood IllnessCAREZAMBIAОценок пока нет
- Cummunity Health Nursing Ii: Study Plan/Checklist (Tal)Документ3 страницыCummunity Health Nursing Ii: Study Plan/Checklist (Tal)ライОценок пока нет
- The Five Level of LeadershipДокумент35 страницThe Five Level of LeadershipNazzil SaifuddinОценок пока нет
- Seizures in Children JULIO 2020Документ29 страницSeizures in Children JULIO 2020Elizabeth HendersonОценок пока нет
- StreptococciДокумент91 страницаStreptococciDr. Ashish JawarkarОценок пока нет
- 14 - Understanding Autism PowerPoint ShowДокумент30 страниц14 - Understanding Autism PowerPoint Showdrammaldzulfiqar IsmailОценок пока нет
- Class Indications Available Dosage Form in The Hospital: AtosibanДокумент2 страницыClass Indications Available Dosage Form in The Hospital: AtosibanDhanu GaysonsiriОценок пока нет
- Mental Capital SummaryДокумент52 страницыMental Capital SummaryaguzzzОценок пока нет
- Breast Cancer Content Concepts Map For Case Study1Документ3 страницыBreast Cancer Content Concepts Map For Case Study1akankshaОценок пока нет
- Bells PalsyДокумент18 страницBells PalsyDr AnandОценок пока нет
- Assessment Planning and Implementation Evaluation: Subjective Data: STG: STGДокумент3 страницыAssessment Planning and Implementation Evaluation: Subjective Data: STG: STGJoel Nick Molano100% (1)
- Action Against Hunger:: Acute Malnutrition BrochureДокумент7 страницAction Against Hunger:: Acute Malnutrition BrochureAction Against Hunger USA100% (1)
- Nursing Care Plans for Febrile Seizures in ChildrenДокумент16 страницNursing Care Plans for Febrile Seizures in ChildrenRedgina CalimlimОценок пока нет
- Basic Metabolic Panel-5Документ1 страницаBasic Metabolic Panel-5dr9348345000Оценок пока нет
- Stree Cardiomyopathy-23Документ7 страницStree Cardiomyopathy-23dr9348345000Оценок пока нет
- Basic Metabolic Panel-5Документ1 страницаBasic Metabolic Panel-5dr9348345000Оценок пока нет
- Basic Metabolic Panel-9Документ1 страницаBasic Metabolic Panel-9dr9348345000Оценок пока нет
- Insulin Tharapy 1Документ11 страницInsulin Tharapy 1dr9348345000Оценок пока нет
- Bionica PumpДокумент19 страницBionica Pumpdr9348345000Оценок пока нет
- Cellular Activation Therapy-ProtocolДокумент4 страницыCellular Activation Therapy-Protocoldr9348345000Оценок пока нет
- CAT Therapy PresentationДокумент18 страницCAT Therapy PresentationNag Mallesh RaoОценок пока нет
- Nmrao ResumeДокумент5 страницNmrao Resumedr9348345000Оценок пока нет
- Basic Metabolic Panel-5Документ1 страницаBasic Metabolic Panel-5dr9348345000Оценок пока нет
- Cariospec Physician BrochureДокумент6 страницCariospec Physician Brochuredr9348345000Оценок пока нет
- Cat TherapyДокумент14 страницCat Therapydr9348345000Оценок пока нет
- Cariospec Physician BrochureДокумент6 страницCariospec Physician Brochuredr9348345000Оценок пока нет
- GEHealthcare Brochure Discovery MR750w3 0TДокумент20 страницGEHealthcare Brochure Discovery MR750w3 0Tdr9348345000Оценок пока нет
- ChitiДокумент2 страницыChitidr9348345000Оценок пока нет
- Heart Failure Society of KhammamДокумент2 страницыHeart Failure Society of Khammamdr9348345000Оценок пока нет
- Echocardiography To Estimate PV Resistance PDFДокумент10 страницEchocardiography To Estimate PV Resistance PDFdr9348345000Оценок пока нет
- 24 The Bladder MeridianДокумент44 страницы24 The Bladder Meridiandr9348345000Оценок пока нет
- Diastolic Heart FailureДокумент5 страницDiastolic Heart Failuredr9348345000Оценок пока нет
- Cardiac Defibrillation Mechanisms Challenges and Implications PDFДокумент260 страницCardiac Defibrillation Mechanisms Challenges and Implications PDFdr9348345000100% (1)
- Pain ManagementДокумент32 страницыPain Managementdr9348345000Оценок пока нет
- Pain ManagementДокумент32 страницыPain Managementdr9348345000Оценок пока нет
- Detox Lazy Way To Perfec HealthДокумент193 страницыDetox Lazy Way To Perfec Healthdr9348345000100% (2)
- 24 The Bladder MeridianДокумент44 страницы24 The Bladder Meridiandr9348345000Оценок пока нет
- Expression of MDM2 and p16 in AngiomyolipomaДокумент7 страницExpression of MDM2 and p16 in AngiomyolipomaTiago TavaresОценок пока нет
- 19 Spinal CordДокумент8 страниц19 Spinal Cordkarar AhmedОценок пока нет
- Complications of 3rd TrimesterДокумент49 страницComplications of 3rd TrimesterMA. JYRELL BONITOОценок пока нет
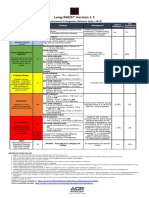
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Документ1 страницаLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotОценок пока нет
- Myocardial InfarctionДокумент18 страницMyocardial InfarctionMarc Lorenz DucusinОценок пока нет
- 13 - Adverse Drug Reactions CausesДокумент4 страницы13 - Adverse Drug Reactions CausesRojas Evert AlonsoОценок пока нет
- Dementia Incidence, Burden and Cost of Care: A Filipino Community-Based StudyДокумент9 страницDementia Incidence, Burden and Cost of Care: A Filipino Community-Based StudyVanessa PalomaОценок пока нет
- Elevated Serum Immunoglobulin E Level As A Marker For Progression Ofimmunoglobulin A NephropathyДокумент5 страницElevated Serum Immunoglobulin E Level As A Marker For Progression Ofimmunoglobulin A Nephropathyagustinaw1981Оценок пока нет
- Full Body To Body Massage Centre in MG Road Gurgaon Delhi NCRДокумент11 страницFull Body To Body Massage Centre in MG Road Gurgaon Delhi NCRFlip Body SpaОценок пока нет
- Autism and Dietary Therapy: Case Report and Review of The LiteratureДокумент6 страницAutism and Dietary Therapy: Case Report and Review of The LiteratureAntiopi PanteliОценок пока нет
- CDN 1 PDFДокумент22 страницыCDN 1 PDFJohn Mark100% (1)
- Jomi 7657Документ27 страницJomi 7657casto.carpetasmiaОценок пока нет
- HematologyДокумент100 страницHematologyerzaraptorОценок пока нет
- TimeWise Miracle Set 3D Fact Sheet MYSG ENGДокумент2 страницыTimeWise Miracle Set 3D Fact Sheet MYSG ENGKilinSilinОценок пока нет
- Literature Review Type 2 DiabetesДокумент4 страницыLiterature Review Type 2 Diabetesafmaadalrefplh100% (1)
- List of Empanelled Hospitals in CGHS NagpurДокумент58 страницList of Empanelled Hospitals in CGHS NagpurRajatОценок пока нет
- Critical Thinking Case Study #18:: Sickle-Cell AnemiaДокумент15 страницCritical Thinking Case Study #18:: Sickle-Cell AnemiaHakima Hadji DaudОценок пока нет
- Pathophysiology of Deep Vein Thrombosis (Thrombophlebitis)Документ7 страницPathophysiology of Deep Vein Thrombosis (Thrombophlebitis)resty tacataОценок пока нет
- Diet PlanДокумент6 страницDiet Plantrical27 tricalОценок пока нет
- IV Drug ReactionsДокумент19 страницIV Drug Reactionsphp_czarina04421Оценок пока нет
- Should Medical Marijuana Be Legalized For PatientsДокумент4 страницыShould Medical Marijuana Be Legalized For PatientsBing Cossid Quinones CatzОценок пока нет
- Sleep and The Risk of Chronic Kidney Disease: A Cohort StudyДокумент8 страницSleep and The Risk of Chronic Kidney Disease: A Cohort StudyEtaursaeОценок пока нет
- Community Health and Program Services (CHAPS) : Health Disparities Among Racial/Ethnic PopulationsДокумент4 страницыCommunity Health and Program Services (CHAPS) : Health Disparities Among Racial/Ethnic PopulationsMuhammad Bachiar SafrudinОценок пока нет