Вам также может понравиться
- Trimmed JSW Lakshya 1.0Документ27 страницTrimmed JSW Lakshya 1.0Sutikshna MishraОценок пока нет
- Commission Master For Insurance Products: Insurance Provider: ICICI Prudential Life Insurance Co. LTDДокумент5 страницCommission Master For Insurance Products: Insurance Provider: ICICI Prudential Life Insurance Co. LTDSutikshna MishraОценок пока нет
- Writing Instructional ObjectivesДокумент35 страницWriting Instructional ObjectivesSutikshna MishraОценок пока нет
- Personal Accident: An Investment To Protect Your Family's FutureДокумент4 страницыPersonal Accident: An Investment To Protect Your Family's FutureSutikshna MishraОценок пока нет
- Leader As Coach1Документ3 страницыLeader As Coach1Sutikshna MishraОценок пока нет
- Mock Test QuestionsДокумент15 страницMock Test QuestionsSutikshna MishraОценок пока нет
- Anandam JoyДокумент13 страницAnandam JoySutikshna MishraОценок пока нет
- Interesting Facts in SalesДокумент1 страницаInteresting Facts in SalesSutikshna MishraОценок пока нет
- AO SmithДокумент10 страницAO SmithSutikshna MishraОценок пока нет
- CV - Pulkit Shukla - Doc-1Документ8 страницCV - Pulkit Shukla - Doc-1Sutikshna MishraОценок пока нет
- AO SmithДокумент10 страницAO SmithSutikshna MishraОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
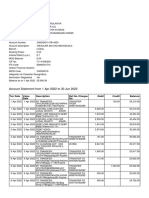
- Account Statement From 1 Apr 2022 To 30 Jun 2022: TXN Date Value Date Description Ref No./Cheque No. Debit Credit BalanceДокумент10 страницAccount Statement From 1 Apr 2022 To 30 Jun 2022: TXN Date Value Date Description Ref No./Cheque No. Debit Credit BalanceParveen SainiОценок пока нет
- Qazi Mohsin Ali: Career ObjectiveДокумент4 страницыQazi Mohsin Ali: Career ObjectiveSamia KhalidОценок пока нет
- Hostel ManualДокумент30 страницHostel ManualpupegufОценок пока нет
- Uniform Loan Delivery Data - Set FaqsДокумент4 страницыUniform Loan Delivery Data - Set FaqsraghuОценок пока нет
- Nature of PostsДокумент13 страницNature of PostsSagargn SagarОценок пока нет
- Banking in India For WbcsДокумент29 страницBanking in India For WbcsSubhasis MaityОценок пока нет
- UK Financial Regulation Ed23-5 PDFДокумент298 страницUK Financial Regulation Ed23-5 PDFVincenzo Somma100% (2)
- Financial Services Project Manager CVДокумент2 страницыFinancial Services Project Manager CVMike KelleyОценок пока нет
- Project On Mutual FundsДокумент86 страницProject On Mutual Fundsmohindrudinit88% (33)
- SOREV Income Approach DiagnosticДокумент4 страницыSOREV Income Approach DiagnosticReyn شكرا100% (1)
- Bajaj Finserv (BAFINS) : Finance Momentum Strong Life Picks UpДокумент12 страницBajaj Finserv (BAFINS) : Finance Momentum Strong Life Picks Uparun_algoОценок пока нет
- Maths ProjectДокумент15 страницMaths Projecttmbcreditdummy50% (2)
- Retail Loan Rates Comparision Chart PDFДокумент3 страницыRetail Loan Rates Comparision Chart PDF9778486995Оценок пока нет
- Collaborative Consumption With Rachel BotsmanДокумент28 страницCollaborative Consumption With Rachel BotsmanSeokwon Yang100% (1)
- Madoff's American Express Corporate Card StatementДокумент30 страницMadoff's American Express Corporate Card StatementInvestor Protection100% (3)
- Barkatullah Vishwavidyalaya Migration Cert - Format FilledupДокумент5 страницBarkatullah Vishwavidyalaya Migration Cert - Format FilledupRojukurthi SudhakarОценок пока нет
- Chap 002 NotesДокумент43 страницыChap 002 NotessamiullahaslamОценок пока нет
- Chapter 13 The Human Resources Management and Payroll CycleДокумент67 страницChapter 13 The Human Resources Management and Payroll CycleislamelshahatОценок пока нет
- Code Movement Sub Movement Code Number SourceДокумент44 страницыCode Movement Sub Movement Code Number SourceSanath SuvarnaОценок пока нет
- Shwethacoffee11 PDFДокумент6 страницShwethacoffee11 PDFabhilash eshwarappaОценок пока нет
- Xtreme Dance January Newsletter 2012Документ1 страницаXtreme Dance January Newsletter 2012incontroltechОценок пока нет
- BillSTMT 4588260000514267Документ3 страницыBillSTMT 4588260000514267Fahad AhmedОценок пока нет
- A Study On Customers Satisfaction-1102-With-cover-page-V2 Ex ProjectДокумент16 страницA Study On Customers Satisfaction-1102-With-cover-page-V2 Ex ProjectFelix ChristoferОценок пока нет
- Loans User Manual PDFДокумент600 страницLoans User Manual PDFdevarchitОценок пока нет
- Case Study - 6: TITLE: Corporate Failure (Money Laundering)Документ7 страницCase Study - 6: TITLE: Corporate Failure (Money Laundering)KanakaMaha LakshmiОценок пока нет
- Case 11 A LBP V RiveraДокумент8 страницCase 11 A LBP V RiveraNathalie YapОценок пока нет
- Internship Report Format For UIMSДокумент17 страницInternship Report Format For UIMSasimkhan2014Оценок пока нет
- Payment Process Request Status ReportДокумент1 страницаPayment Process Request Status ReportNishant RanaОценок пока нет
- Chinese Busssines ReviewДокумент136 страницChinese Busssines Reviewamir hamzahОценок пока нет
- Forms of Registration Under Contract Labour Act 1970 PDFДокумент7 страницForms of Registration Under Contract Labour Act 1970 PDFGlendaОценок пока нет