Вам также может понравиться
- Meningitis and Encephalitis: Causes, Symptoms and TreatmentsДокумент71 страницаMeningitis and Encephalitis: Causes, Symptoms and TreatmentsKaif KhanОценок пока нет
- Encephalitis Causes, Symptoms & DiagnosisДокумент55 страницEncephalitis Causes, Symptoms & DiagnosisAmit MartinОценок пока нет
- BronchiolitisДокумент7 страницBronchiolitisNader SmadiОценок пока нет
- Hypoxic Ischemic EncephalopathyДокумент7 страницHypoxic Ischemic EncephalopathyJennesse May Guiao IbayОценок пока нет
- Neonatal SepsisДокумент63 страницыNeonatal SepsisDemewoz Fikir100% (1)
- Neonatal Hypocalcemia: Presented By: Ms. Manisha Thakur Nursing Tutor Child Health NursingДокумент11 страницNeonatal Hypocalcemia: Presented By: Ms. Manisha Thakur Nursing Tutor Child Health Nursingmanisha thakurОценок пока нет
- Congenital Malformations of The Nervous System PDFДокумент16 страницCongenital Malformations of The Nervous System PDFPriyanjali SainiОценок пока нет
- ENCEPHALITISДокумент37 страницENCEPHALITISNida NaazОценок пока нет
- Care of Preterm Babies FinalДокумент33 страницыCare of Preterm Babies Finalchinchu100% (1)
- Meconium Aspiration SyndromeДокумент26 страницMeconium Aspiration SyndromeJOSLIN100% (2)
- Hirschsprung Disease (Aganglionic Megacolon)Документ6 страницHirschsprung Disease (Aganglionic Megacolon)Julliza Joy PandiОценок пока нет
- Congenital AnomaliesДокумент94 страницыCongenital AnomaliesDeepti Kukreti100% (1)
- Meconium Stained Amniotic FluidДокумент21 страницаMeconium Stained Amniotic FluidPoonam RanaОценок пока нет
- Ophthalmia NeonatorumДокумент30 страницOphthalmia NeonatorumManish ShresthaОценок пока нет
- Assessing Preterm BabyДокумент5 страницAssessing Preterm BabyJoyce Kathreen Ebio LopezОценок пока нет
- Care of Preterm Babies GuideДокумент59 страницCare of Preterm Babies GuideChinchu MohanОценок пока нет
- Seminar On Bronchial Asthma NewДокумент42 страницыSeminar On Bronchial Asthma NewShabna SameerОценок пока нет
- Tetralogy of FallotДокумент10 страницTetralogy of FallotanggiehardiyantiОценок пока нет
- Encephalitis: - Gunaseelan KumarДокумент30 страницEncephalitis: - Gunaseelan KumarGunaseelan Kumar100% (1)
- HydrocephalusДокумент21 страницаHydrocephalusprecillathoppil100% (1)
- Hiv and Aids in ChildrenДокумент36 страницHiv and Aids in ChildrenKazau FwalangaОценок пока нет
- CVAДокумент16 страницCVANithiy TОценок пока нет
- Spina Bifida: Causes, Types and TreatmentДокумент17 страницSpina Bifida: Causes, Types and Treatmentjessy100% (1)
- Hypoxic Ischemic EncephalopathyДокумент13 страницHypoxic Ischemic Encephalopathyscribdkhasa100% (1)
- Nursing Theory ApplicationДокумент16 страницNursing Theory ApplicationAnusha VergheseОценок пока нет
- CcroupДокумент53 страницыCcroupOlivia BernadiОценок пока нет
- Birth Injuries PDFДокумент24 страницыBirth Injuries PDFsaritha OrugantiОценок пока нет
- Presented By: Gayramara Arben John ZДокумент36 страницPresented By: Gayramara Arben John ZgoykicoshenОценок пока нет
- Meningocele & Spina BifidaДокумент20 страницMeningocele & Spina BifidaAstrid SabirinОценок пока нет
- EncephalitisДокумент33 страницыEncephalitisJona de VeraОценок пока нет
- TetanusДокумент23 страницыTetanusDhynie Soesila WahyudiОценок пока нет
- Care unconscious clientsДокумент27 страницCare unconscious clientsDonelie Kay Tapel AsanzaОценок пока нет
- Care of Unconscious PatientДокумент6 страницCare of Unconscious PatientSuparna SinghaОценок пока нет
- Adjustment Reaction To SchoolДокумент6 страницAdjustment Reaction To SchoolYatharth DateerОценок пока нет
- Meningitis (Completed)Документ26 страницMeningitis (Completed)seema83% (6)
- Pulmonary TuberculosisДокумент17 страницPulmonary TuberculosisRobert Dominic GonzalesОценок пока нет
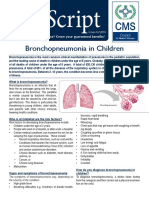
- Bronchopneumonia in ChildrenДокумент3 страницыBronchopneumonia in ChildrenputraОценок пока нет
- Guillain Barre Syndrome (GBS) ImanДокумент26 страницGuillain Barre Syndrome (GBS) ImanTowardsLight100% (5)
- Presentation on Guillain-Barre SyndromeДокумент12 страницPresentation on Guillain-Barre Syndromepandem soniyaОценок пока нет
- Neonatal Eye Infection Guide: Causes, Tests & TreatmentsДокумент17 страницNeonatal Eye Infection Guide: Causes, Tests & TreatmentsIndranil DuttaОценок пока нет
- Hospitalization: Meaning of Hospitalization:-" DefinitionДокумент12 страницHospitalization: Meaning of Hospitalization:-" DefinitionPriyaОценок пока нет
- Child With Blood DisorderДокумент126 страницChild With Blood DisorderSivabarathyОценок пока нет
- What Is Spina BifidaДокумент18 страницWhat Is Spina BifidaAnonymous dI1hgIJfjzОценок пока нет
- HypothermiaДокумент5 страницHypothermiaMRS CHAKRAPANIОценок пока нет
- 5 Bronchiolitis Nursing Care Plans - NurseslabsДокумент14 страниц5 Bronchiolitis Nursing Care Plans - NurseslabsAnnapoorna SHОценок пока нет
- My - Failure To ThriveДокумент31 страницаMy - Failure To ThriveAuliaRahman100% (1)
- Congenital Anomalies of Skeletal SystemДокумент44 страницыCongenital Anomalies of Skeletal SystemMeena Koushal100% (1)
- Cerebrovascular AccidentДокумент21 страницаCerebrovascular AccidentCJОценок пока нет
- K6 - Tetanus PEDIATRICДокумент23 страницыK6 - Tetanus PEDIATRICbanuperiahОценок пока нет
- Neonatal SepsisДокумент8 страницNeonatal Sepsis+nellaОценок пока нет
- Nicu DoccumentationДокумент17 страницNicu Doccumentationchaarvi100% (1)
- Guillian Barre SyndromeДокумент6 страницGuillian Barre SyndromeRhomz Zubieta RamirezОценок пока нет
- Retinal DetachmentДокумент6 страницRetinal DetachmentNader Smadi100% (3)
- MENINGITISДокумент44 страницыMENINGITIStummalapalli venkateswara rao100% (5)
- Classroom Teaching on TetanusДокумент17 страницClassroom Teaching on TetanusT. Chang100% (1)
- Neurological InfectionsДокумент21 страницаNeurological Infectionsfortuneholiness11Оценок пока нет
- Meningitis &encephalitisДокумент9 страницMeningitis &encephalitisSnIP StandredОценок пока нет
- Neurological Infections: Gerard Gabriel P. Reotutar, RM, RN, MANДокумент33 страницыNeurological Infections: Gerard Gabriel P. Reotutar, RM, RN, MANJeremiash Noblesala Dela CruzОценок пока нет
- Acute Bacterial MeningitisДокумент15 страницAcute Bacterial MeningitisOana StefanОценок пока нет
- PRADEEP'S GlaucomaДокумент33 страницыPRADEEP'S GlaucomaPRADEEPОценок пока нет
- PRADEEP'S - Acute BronchitisДокумент15 страницPRADEEP'S - Acute BronchitisPRADEEPОценок пока нет
- PRADEEP'S - Acute BronchitisДокумент15 страницPRADEEP'S - Acute BronchitisPRADEEPОценок пока нет
- PRADEEP'S - AnginaДокумент35 страницPRADEEP'S - AnginaPRADEEPОценок пока нет
- PRADEEP'S - CommunicationДокумент30 страницPRADEEP'S - CommunicationPRADEEP100% (1)
- PRADEEP'S - Preparation and Use PF Non-Projected A-V AidsДокумент38 страницPRADEEP'S - Preparation and Use PF Non-Projected A-V AidsPRADEEPОценок пока нет
- PRADEEP'S - Brain TumorДокумент32 страницыPRADEEP'S - Brain TumorPRADEEPОценок пока нет
- Diversity QuotasДокумент7 страницDiversity Quotasapi-609564626Оценок пока нет
- SFNHS - Extension's School Learning Continuity PlanДокумент5 страницSFNHS - Extension's School Learning Continuity PlanClaudie MabiniОценок пока нет
- Yuken pvr50 FF 45 Raa 3180 Hydraulic Vane PumpДокумент4 страницыYuken pvr50 FF 45 Raa 3180 Hydraulic Vane Pumpnelson nadarОценок пока нет
- USI Pakistan Program-A Successs StoryДокумент4 страницыUSI Pakistan Program-A Successs StoryThomas CannonОценок пока нет
- The Liver in Systemic Disease A Clinician's Guide To Abnormal LiverДокумент285 страницThe Liver in Systemic Disease A Clinician's Guide To Abnormal Liveroleksandra.bilotkachОценок пока нет
- LDRRMPДокумент39 страницLDRRMPMarlon VillenaОценок пока нет
- Clinical Review - KEDRABДокумент97 страницClinical Review - KEDRABcoolchapОценок пока нет
- FP02BДокумент3 страницыFP02BRazak JeyОценок пока нет
- Management of BurnДокумент42 страницыManagement of BurnArisa KudidthalertОценок пока нет
- HRM Questionnaire HR Functions SurveyДокумент6 страницHRM Questionnaire HR Functions SurveyMagendran Adeyah67% (3)
- The Dolphin: by Sergio Bambarén. Maritza - Jhunior - Cynthia - Carlos - AlexДокумент10 страницThe Dolphin: by Sergio Bambarén. Maritza - Jhunior - Cynthia - Carlos - AlexAlexandra FlorОценок пока нет
- LakesДокумент14 страницLakesmanwartejam8Оценок пока нет
- Elkefi Et Al 2022 Impact of Health Informatics On Patients Perception of Health Care Services Trends Over Time ofДокумент6 страницElkefi Et Al 2022 Impact of Health Informatics On Patients Perception of Health Care Services Trends Over Time ofeva kacanjaОценок пока нет
- Class 8 Physics 3Документ16 страницClass 8 Physics 3Akhil ChintalapalliОценок пока нет
- Jim106 Chapter 1 Practice ExercisesДокумент3 страницыJim106 Chapter 1 Practice ExercisesHor KaiОценок пока нет
- Operation and Maintenance of Power PlantДокумент31 страницаOperation and Maintenance of Power PlantAnkur Pathak100% (1)
- 2 Ways To Check Your Pulse - WikiHowДокумент2 страницы2 Ways To Check Your Pulse - WikiHowRalph JohnsonОценок пока нет
- ATEX Guidelines for the Valve IndustryДокумент49 страницATEX Guidelines for the Valve Industryio1_roОценок пока нет
- Dissolvine 100-S MSDSДокумент8 страницDissolvine 100-S MSDSMichaelОценок пока нет
- Artículo Estudio Ramachandran AGI Personas Bigénero PDFДокумент6 страницArtículo Estudio Ramachandran AGI Personas Bigénero PDFMikaОценок пока нет
- Ielts. Writing Task 1. ExamplesДокумент3 страницыIelts. Writing Task 1. Examplestatianafl08Оценок пока нет
- Nadilla Choerunnisa 2B S.KepДокумент3 страницыNadilla Choerunnisa 2B S.KepNadilla ChoerunnisaОценок пока нет
- Flowers From 1970Документ93 страницыFlowers From 1970isla62% (21)
- Sterilization and DisinfectionДокумент41 страницаSterilization and DisinfectionqiotenseiОценок пока нет
- General Biology 1: Quarter 1 - Module - : Title: Cell CycleДокумент27 страницGeneral Biology 1: Quarter 1 - Module - : Title: Cell CycleRea A. Bilan0% (1)
- Republic of The Philippines: Cavite State University Don Severino de Las Alas CampusДокумент5 страницRepublic of The Philippines: Cavite State University Don Severino de Las Alas CampusRobin EscosesОценок пока нет
- All India Test Series (2023-24)Документ22 страницыAll India Test Series (2023-24)Anil KumarОценок пока нет
- Anaphylaxis and Epinephrine Auto-InjectorДокумент7 страницAnaphylaxis and Epinephrine Auto-Injectorqueennita69Оценок пока нет
- Lecture 2Документ8 страницLecture 2salmanqaadirОценок пока нет
- Processing Cacao Pod Husk into Low-Methoxyl PectinДокумент9 страницProcessing Cacao Pod Husk into Low-Methoxyl PectinEmmanuel PlazaОценок пока нет