Вам также может понравиться
- ENT History TakingДокумент14 страницENT History TakingST67% (3)
- ParasitologyДокумент18 страницParasitologyLudwig359100% (2)
- ENT DiseasesДокумент75 страницENT DiseasesGudeta shegerОценок пока нет
- Ears, Nose and Throat Diseases: Prepared By: Hannelli BelingonДокумент103 страницыEars, Nose and Throat Diseases: Prepared By: Hannelli BelingonPatricia Kamille I. PawidОценок пока нет
- Chronic Otitis Media Types, Investigations, TreatmentДокумент43 страницыChronic Otitis Media Types, Investigations, TreatmentPrasanna DattaОценок пока нет
- CSOMДокумент74 страницыCSOMSunil KumarОценок пока нет
- Common ENT Conditions PresentationДокумент60 страницCommon ENT Conditions PresentationMICHAEL SAKALAОценок пока нет
- AA CsomДокумент31 страницаAA Csomnahidanila439Оценок пока нет
- ASOMДокумент53 страницыASOMAyman YakoutОценок пока нет
- Lecture 2.1-External Ear Disorders-Ashadi Prasetyo (2017) PDFДокумент71 страницаLecture 2.1-External Ear Disorders-Ashadi Prasetyo (2017) PDFAnonymous XFDJfsGviОценок пока нет
- Csom Atticoantral (Modified)Документ24 страницыCsom Atticoantral (Modified)Muhammad MunawarОценок пока нет
- Group 11 MastoiditisДокумент23 страницыGroup 11 MastoiditisYen-Naah AdamsОценок пока нет
- The Ear and It's DisordersДокумент104 страницыThe Ear and It's DisordersAyaBasilioОценок пока нет
- Infeksi Telinga: Rizka Dany AfinaДокумент63 страницыInfeksi Telinga: Rizka Dany AfinaRizka Dany AfinaОценок пока нет
- Diseases of The EarДокумент48 страницDiseases of The Earabela_amulu100% (1)
- Kuliah Tuli Konduktif Infeksi TelingaДокумент66 страницKuliah Tuli Konduktif Infeksi TelingaRizka Dany AfinaОценок пока нет
- Symptom A To Logy of EarДокумент36 страницSymptom A To Logy of Ear98480sam23006100% (1)
- Middle Ear CHR DiseasesДокумент157 страницMiddle Ear CHR DiseasesAdi SitaruОценок пока нет
- Ryan Martin Ko, M.DДокумент54 страницыRyan Martin Ko, M.DDhaval Makwana100% (2)
- CSOM of Middle Ear Part 1Документ59 страницCSOM of Middle Ear Part 1Anindya Nandi100% (1)
- tham khảo cholesteatoma bone pate PDFДокумент35 страницtham khảo cholesteatoma bone pate PDFdaohailongОценок пока нет
- Pathophysiology and Complications of CSOMДокумент42 страницыPathophysiology and Complications of CSOMSalsabilla Ameranti PutriОценок пока нет
- OtitisanДокумент54 страницыOtitisanmagreaОценок пока нет
- Otitis MediaДокумент32 страницыOtitis MediaRiya GautamОценок пока нет
- Otitis MediaДокумент11 страницOtitis MediaAnkita BramheОценок пока нет
- 03.chronic Supp Otitis MediaДокумент33 страницы03.chronic Supp Otitis MediaJumanne JayОценок пока нет
- External Ear Pathology - PresentationДокумент25 страницExternal Ear Pathology - PresentationNipun MalhotraОценок пока нет
- Chronic Suppurative Otitis Media (CSOM)Документ31 страницаChronic Suppurative Otitis Media (CSOM)Mimo HemadОценок пока нет
- 2 Otitis MediaДокумент19 страниц2 Otitis MediaAparna SinghОценок пока нет
- EarДокумент123 страницыEarAvlya ZelykaОценок пока нет
- SM Calmed ... Chronic Otitis Media - Squamosal DiseaseДокумент53 страницыSM Calmed ... Chronic Otitis Media - Squamosal DiseaseanisОценок пока нет
- CSOM of Middle Ear Part 2Документ55 страницCSOM of Middle Ear Part 2Anindya NandiОценок пока нет
- Davao Medical School Foundation: Chris Robinson D. Laganao, MD, DPBO-HNSДокумент48 страницDavao Medical School Foundation: Chris Robinson D. Laganao, MD, DPBO-HNSVasiliás PrawinОценок пока нет
- Chronic Suppurative Otitis Media: Drhpsingh Additional ProfessorДокумент44 страницыChronic Suppurative Otitis Media: Drhpsingh Additional ProfessorIndieОценок пока нет
- Cholesteatoma: Clinical Features Diagnosis TreatmentДокумент19 страницCholesteatoma: Clinical Features Diagnosis TreatmentDoodОценок пока нет
- Complications of Suppurative Otitis MediaДокумент21 страницаComplications of Suppurative Otitis MediaSalsabila Al-BasheerОценок пока нет
- Common Ent DisordersДокумент20 страницCommon Ent DisordersattaheeraОценок пока нет
- Diseasesofexternalear 1Документ86 страницDiseasesofexternalear 1Nitin Sharma100% (1)
- CholesteotomaДокумент33 страницыCholesteotomaWael ShamyОценок пока нет
- Kuliah THT FKUI TK 4 Kapita SelektaДокумент39 страницKuliah THT FKUI TK 4 Kapita SelektaSri HartatiОценок пока нет
- Otitis MediaДокумент98 страницOtitis MediaLody Lean CruzОценок пока нет
- CSOMДокумент50 страницCSOMFurqan MirzaОценок пока нет
- 1-Causes of Hearing ImpairmentДокумент28 страниц1-Causes of Hearing Impairmentjohn mwambuОценок пока нет
- Ent Past Years Question According To TopicsДокумент32 страницыEnt Past Years Question According To Topicsmohamed100% (1)
- Csom TTДокумент24 страницыCsom TTnahidanila439Оценок пока нет
- Middle Ear Diseases by Prof Mahmoud AttiaДокумент84 страницыMiddle Ear Diseases by Prof Mahmoud AttiaWesam TayaОценок пока нет
- Ear DischargeДокумент69 страницEar DischargeNabylah YutakaОценок пока нет
- ENT Lectures 1Документ123 страницыENT Lectures 1lxnalexander100% (1)
- Otitis Media: Prepared By: - Priyanka ThapaДокумент38 страницOtitis Media: Prepared By: - Priyanka ThapaKalo kajiОценок пока нет
- Drugs and Substance AbuseДокумент75 страницDrugs and Substance Abuseseline sherylОценок пока нет
- CsoomДокумент18 страницCsoomibrahimdarsОценок пока нет
- Acute Otitis Media: Dr. Ajay Manickam Junior Resident RG Kar Medical College HospitalДокумент20 страницAcute Otitis Media: Dr. Ajay Manickam Junior Resident RG Kar Medical College HospitalchawkatОценок пока нет
- CSOMДокумент29 страницCSOMsuciОценок пока нет
- Presentations of Middle Ear Disease: Elizabeth Rose Royal Victorian Eye and Ear Hospital Royal Children's HospitalДокумент43 страницыPresentations of Middle Ear Disease: Elizabeth Rose Royal Victorian Eye and Ear Hospital Royal Children's Hospitalathe_triiaОценок пока нет
- Lecture 2 Ent.Документ70 страницLecture 2 Ent.kiprotich weldonОценок пока нет
- CholesteatomaДокумент30 страницCholesteatoma李丞永Оценок пока нет
- Oro-Antral CommunicationДокумент65 страницOro-Antral CommunicationNadila RОценок пока нет
- Clinical Features and DiagnosisДокумент9 страницClinical Features and DiagnosisSaifulAizatОценок пока нет
- Cholesteatoma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandCholesteatoma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- OHNS--Otolaryngology; Head and Neck surgery: pocket field guideОт EverandOHNS--Otolaryngology; Head and Neck surgery: pocket field guideОценок пока нет
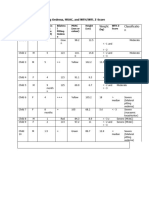
- PART C. Bilateral Pitting Oedema, MUAC, and WFH/WFL Z-Score: Weight Classificatio NДокумент12 страницPART C. Bilateral Pitting Oedema, MUAC, and WFH/WFL Z-Score: Weight Classificatio NFeiruzОценок пока нет
- Chapter 4 Drug StudyДокумент9 страницChapter 4 Drug StudyRegee Rose LacsonОценок пока нет
- Biology Project: Made By:-Swasti Tyagi, Xii-A, 25Документ18 страницBiology Project: Made By:-Swasti Tyagi, Xii-A, 25Swasti TyagiОценок пока нет
- Tuberculosis in Infancy and ChildhoodДокумент32 страницыTuberculosis in Infancy and ChildhoodArvin E. PamatianОценок пока нет
- Infection ControlДокумент3 страницыInfection ControlHazelina VillamorОценок пока нет
- SVN 078 - 2021 - Migration Health Nurse II, Jakarta - 1Документ4 страницыSVN 078 - 2021 - Migration Health Nurse II, Jakarta - 1agnes febriyantiОценок пока нет
- A Critique On The Film Contagion - HardДокумент2 страницыA Critique On The Film Contagion - HardEchoОценок пока нет
- Modl Paper - Infection ControlДокумент2 страницыModl Paper - Infection ControlSaima ParveenОценок пока нет
- Hepa B Vaccine Consent FormДокумент2 страницыHepa B Vaccine Consent FormKESLEY DELOS SANTOSОценок пока нет
- WHO 2019 nCoV Vaccine Effectiveness Measurement 2021.1 EngДокумент70 страницWHO 2019 nCoV Vaccine Effectiveness Measurement 2021.1 EngChio MoranteОценок пока нет
- Dog Bite ManagementДокумент94 страницыDog Bite ManagementHari Krishnan ElangovanОценок пока нет
- Dengue IGG IGM X 10 All TestДокумент1 страницаDengue IGG IGM X 10 All TestKaren Ramos CardenasОценок пока нет
- DSBDA Covid - CasesДокумент11 страницDSBDA Covid - CasesdanawaleharshadОценок пока нет
- PDS - Metazolone-FM - Ver 2.0Документ1 страницаPDS - Metazolone-FM - Ver 2.0Rama KrishnanОценок пока нет
- Colloidal Silver and ShinglesДокумент7 страницColloidal Silver and ShinglesduhitijeloОценок пока нет
- Burton's Microbiology Chapter 1Документ3 страницыBurton's Microbiology Chapter 1Micole Paz LopezОценок пока нет
- Intro BacteriaДокумент47 страницIntro BacteriaMj BrionesОценок пока нет
- Azizul Hakim Bin Ramli - 2020605136Документ5 страницAzizul Hakim Bin Ramli - 2020605136MOHD MU'IZZ BIN MOHD SHUKRIОценок пока нет
- MEASLES and MALARIAДокумент19 страницMEASLES and MALARIADoreen Claire M. WallangОценок пока нет
- Nursing Seminar 1 SAS Session 16Документ8 страницNursing Seminar 1 SAS Session 16ZiaОценок пока нет
- Q3 Health 8 Module 1 PDFДокумент15 страницQ3 Health 8 Module 1 PDFkateОценок пока нет
- IOGP 397 Food and Water Safety in The Oil and Gas IndustryДокумент74 страницыIOGP 397 Food and Water Safety in The Oil and Gas IndustryFelicia ErikaОценок пока нет
- Essential Oil Composition and Antimicrobial Interactions of Understudied Tea Tree SpeciesДокумент8 страницEssential Oil Composition and Antimicrobial Interactions of Understudied Tea Tree SpeciesxiuhtlaltzinОценок пока нет
- Erythema MultiformeДокумент3 страницыErythema MultiformeSlim SaaryОценок пока нет
- Joseph ListerДокумент9 страницJoseph ListerIdzhamReezaОценок пока нет
- CHN Pnle Board Exam Practice-Part 4Документ6 страницCHN Pnle Board Exam Practice-Part 4jerarddaria.elakОценок пока нет
- Sunshine Vitamin D Found To Speed Tuberculosis Recovery: Antibiotic Treatment Lung DiseaseДокумент2 страницыSunshine Vitamin D Found To Speed Tuberculosis Recovery: Antibiotic Treatment Lung DiseaseKimsha ConcepcionОценок пока нет
- Slide Kuliah Infectious DiareДокумент75 страницSlide Kuliah Infectious DiareFany Raihan PadilahОценок пока нет
- BookДокумент851 страницаBookJavier Guedeja-Marrón Peinado100% (1)