Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Lord of The Flies AnalysisДокумент10 страницLord of The Flies AnalysisMuhammad AsifОценок пока нет
- A Descriptive-Comparative StudyДокумент32 страницыA Descriptive-Comparative StudyJanelle DionisioОценок пока нет
- Handouts For Module 1 Introduction To EthicsДокумент36 страницHandouts For Module 1 Introduction To EthicsZerimar Dela CruzОценок пока нет
- HG G2 Q1 W57 Module 3 RTPДокумент11 страницHG G2 Q1 W57 Module 3 RTPJennilyn Amable Democrito100% (1)
- Micro Analysis Report - Int1Документ3 страницыMicro Analysis Report - Int1kousikkumaarОценок пока нет
- Theology NotesДокумент3 страницыTheology NotesNia De GuzmanОценок пока нет
- Safety Management in Coromandel FertilizerДокумент7 страницSafety Management in Coromandel FertilizerS Bharadwaj ReddyОценок пока нет
- Syllabus Tourism Laws CKSCДокумент6 страницSyllabus Tourism Laws CKSCDennis Go50% (2)
- Baby Romper Pattern and Sewing Tutorial 2014Документ18 страницBaby Romper Pattern and Sewing Tutorial 2014Carolina Ribeiro100% (1)
- Micro Fibra Sintetica at 06-MapeiДокумент2 страницыMicro Fibra Sintetica at 06-MapeiSergio GonzalezОценок пока нет
- Introduction To Human Resources ManagementДокумент14 страницIntroduction To Human Resources ManagementEvan NoorОценок пока нет
- Lease of Playground To A SchoolДокумент2 страницыLease of Playground To A SchoolSutapaОценок пока нет
- Principle of ManagementsДокумент77 страницPrinciple of ManagementsJayson LucenaОценок пока нет
- WLP Math Week 4 Q4Документ4 страницыWLP Math Week 4 Q4JUDELYN O. DOMINGOОценок пока нет
- The Study of Zooplankton Community Diversity in Zaghen Restored WetlandДокумент6 страницThe Study of Zooplankton Community Diversity in Zaghen Restored WetlandAlexandra GeorgianaОценок пока нет
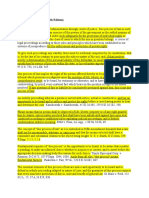
- Due Process of LawДокумент2 страницыDue Process of Lawjoe100% (4)
- Forum Discussion #7 UtilitarianismДокумент3 страницыForum Discussion #7 UtilitarianismLisel SalibioОценок пока нет
- RRLДокумент4 страницыRRLElaine Lacandula100% (1)
- The Java Collections Framework: InterfacesДокумент22 страницыThe Java Collections Framework: InterfacesSourav DasОценок пока нет
- The Basics of Effective Interpersonal Communication: by Sushila BahlДокумент48 страницThe Basics of Effective Interpersonal Communication: by Sushila BahlDevesh KhannaОценок пока нет
- Vince - Michael - Intermediate - Language Assive 1Документ5 страницVince - Michael - Intermediate - Language Assive 1Николай КолевОценок пока нет
- Exotic - March 2014Документ64 страницыExotic - March 2014Almir Momenth35% (23)
- Mircea Eliade and Ernst Jünger On Human Sacrifice, 1937-1945Документ31 страницаMircea Eliade and Ernst Jünger On Human Sacrifice, 1937-1945Direktor Kile100% (1)
- D2-S1 C Harmony in The Human Being July 23Документ20 страницD2-S1 C Harmony in The Human Being July 23padmaОценок пока нет
- CWTS Narrative ReportДокумент10 страницCWTS Narrative ReportJa Rich100% (1)
- Term Coalition Has Been Derived From The Latin Word 'Coalitio' Which Means To Grow Up TogetherДокумент2 страницыTerm Coalition Has Been Derived From The Latin Word 'Coalitio' Which Means To Grow Up TogetherShree MishraОценок пока нет
- Lampiran 18-Lesson Plan 02Документ5 страницLampiran 18-Lesson Plan 02San Louphlii ThaОценок пока нет
- FinTech and Banking DisruptionДокумент13 страницFinTech and Banking DisruptionMaru MasОценок пока нет
- Discuss Both Views Introduction PracticeДокумент3 страницыDiscuss Both Views Introduction PracticeSang NguyễnОценок пока нет
- SerpılДокумент82 страницыSerpılNurhayat KaripОценок пока нет