Вам также может понравиться
- Lab Report Bacteria CountДокумент5 страницLab Report Bacteria Countsarahyahaya67% (3)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- 1 Priority KeywordДокумент8 страниц1 Priority KeywordKavithaОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Astm C97/C97M-09Документ3 страницыAstm C97/C97M-09Azuriak150% (2)
- Proview TutorialДокумент12 страницProview TutorialManoel NascimentoОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Prediction of Graduate Admission IEEE - 2020Документ6 страницPrediction of Graduate Admission IEEE - 2020Anu RamanujamОценок пока нет
- GenMath11 Q1 Mod26 Domain and Range of Logarithmic Functions 08082020Документ19 страницGenMath11 Q1 Mod26 Domain and Range of Logarithmic Functions 08082020Charity Myrh Pasquin ArzagaОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Completation Inteligent RevistaДокумент9 страницCompletation Inteligent RevistaGabriel Castellon HinojosaОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Identification - of - Vulkan Vulastik-L CouplingsДокумент2 страницыIdentification - of - Vulkan Vulastik-L CouplingsBill NevisОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Prob AnswersДокумент4 страницыProb AnswersDaniel KirovОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- HKV-8 Valve Catalog SPLRДокумент128 страницHKV-8 Valve Catalog SPLRCabrera RodriguezОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- BS DanielДокумент6 страницBS Danielsandy30694Оценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- LatheДокумент74 страницыLatheChandrakantha K100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Binomial Poisson Normal DistributionДокумент9 страницBinomial Poisson Normal DistributionFahim MahmudОценок пока нет
- PhysioEx Ex. 9 Act. 2Документ4 страницыPhysioEx Ex. 9 Act. 2Juvy Anne LozanoОценок пока нет
- Unit 7 Motion Review Sheet AnswersДокумент3 страницыUnit 7 Motion Review Sheet AnswersFlorie Fe Rosario Ortega100% (1)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- BQ 76 PL 102Документ23 страницыBQ 76 PL 102AlexОценок пока нет
- Chapter 1 - Distillation PDFДокумент107 страницChapter 1 - Distillation PDFFatin Natasha NazriОценок пока нет
- 1 Kinetic Molecular TheoryДокумент23 страницы1 Kinetic Molecular TheoryAeron Kurt AcuñaОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Java OOP Arrays and ExceptionsДокумент11 страницJava OOP Arrays and ExceptionsJava OOPОценок пока нет
- Mazda 3Документ5 страницMazda 3Jhony GranadosОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Partial Differential Equations (Pdes)Документ5 страницPartial Differential Equations (Pdes)uploadingpersonОценок пока нет
- PowerPoint Practice Exercise 1 InstructionsДокумент3 страницыPowerPoint Practice Exercise 1 InstructionsErick OumaОценок пока нет
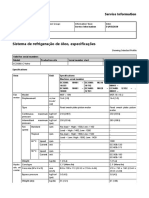
- Sistema de Refrigeração de Óleo, EspecificaçõesДокумент2 страницыSistema de Refrigeração de Óleo, EspecificaçõesAlexandreОценок пока нет
- GP 1 Module 3Документ46 страницGP 1 Module 3Raymund EspinoОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Sap Basis Transaction CodesДокумент2 страницыSap Basis Transaction CodeskatrinbreaksОценок пока нет
- Infinera 7100 Series: Compact and Flexible Packet Optical Transport For The MetroДокумент2 страницыInfinera 7100 Series: Compact and Flexible Packet Optical Transport For The MetroTaha AlhatmiОценок пока нет
- Copeland Discus Digital Compressors Coresense Technology en 2884258Документ2 страницыCopeland Discus Digital Compressors Coresense Technology en 2884258Roberto CastilloОценок пока нет
- MATH 320 Numerical Analysis NotesДокумент70 страницMATH 320 Numerical Analysis NotesWinnie Mutuku100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Susan Abed (2012) - Corporate Governance and Earnings Management Jordanian EvidenceДокумент10 страницSusan Abed (2012) - Corporate Governance and Earnings Management Jordanian Evidenceheryp123Оценок пока нет
- Esam AliДокумент23 страницыEsam AliYoussef AliОценок пока нет