Вам также может понравиться
- Exercise Is Medicine: How To Get You and Your Patients MovingДокумент120 страницExercise Is Medicine: How To Get You and Your Patients MovingMuhammad AbdullahОценок пока нет
- Health and Cycling: Professor Bruce Lynn, UCLДокумент36 страницHealth and Cycling: Professor Bruce Lynn, UCLNadya ShabrinaОценок пока нет
- 1 s2.0 S0735109714027466 MainДокумент10 страниц1 s2.0 S0735109714027466 MainEmail KerjaОценок пока нет
- Essay 2 BibliographyДокумент10 страницEssay 2 Bibliographyapi-579014618Оценок пока нет
- Leitzmann Et Al., (2007) Physical Activity RecommendationsДокумент8 страницLeitzmann Et Al., (2007) Physical Activity RecommendationsAna Flávia SordiОценок пока нет
- Relative Intensity of Physical Activity and Risk of Coronary Heart DiseaseДокумент17 страницRelative Intensity of Physical Activity and Risk of Coronary Heart DiseaseWidya SyahdilaОценок пока нет
- Haskell 2007Документ12 страницHaskell 2007muratigdi96Оценок пока нет
- E.F y AlzheimerДокумент3 страницыE.F y AlzheimerpaoОценок пока нет
- Exercise GuidelineДокумент5 страницExercise GuidelineRina RaehanaОценок пока нет
- Exercice Is MedicineДокумент55 страницExercice Is MedicineDario MoralesОценок пока нет
- mss51270 1324..1339Документ16 страницmss51270 1324..1339matthewquan711Оценок пока нет
- JNC 8 Ala Ala TrustlineДокумент64 страницыJNC 8 Ala Ala TrustlineameliarumentaОценок пока нет
- Research Project-2Документ12 страницResearch Project-2api-663561390Оценок пока нет
- Dietary Protein and Risk of Ischemic Heart Disease in Middle-Aged Men1-3 Sarah Rosner PДокумент8 страницDietary Protein and Risk of Ischemic Heart Disease in Middle-Aged Men1-3 Sarah Rosner Ppaulobrasil.ortopedistaОценок пока нет
- Choosing the StrongPath: Reversing the Downward Spiral of AgingОт EverandChoosing the StrongPath: Reversing the Downward Spiral of AgingРейтинг: 3 из 5 звезд3/5 (2)
- Leisure Time Physical Activity and Mortality A Detailed Pooled Analysis of The Dose-Response RelationshipДокумент9 страницLeisure Time Physical Activity and Mortality A Detailed Pooled Analysis of The Dose-Response RelationshipAgnes Nina EurekaОценок пока нет
- Smoking, Antioxidant Vitamins, and The Risk of Hip FractureДокумент7 страницSmoking, Antioxidant Vitamins, and The Risk of Hip FractureAnonymous pJfAvlОценок пока нет
- The Age Antidote: Len Kravitz, PH.DДокумент6 страницThe Age Antidote: Len Kravitz, PH.D3520952Оценок пока нет
- A Group of 500 Women Whose Health May Depart Notably From The Norm: Protocol For A Cross-Sectional SurveyДокумент12 страницA Group of 500 Women Whose Health May Depart Notably From The Norm: Protocol For A Cross-Sectional Surveyhanna.oravecz1Оценок пока нет
- Physical Health Correlates of Overprediction of Physical Discomfort During ExerciseДокумент14 страницPhysical Health Correlates of Overprediction of Physical Discomfort During ExerciseJaviera Soto AndradeОценок пока нет
- Introduction To Exercise PrescriptionДокумент46 страницIntroduction To Exercise PrescriptionabhijeetОценок пока нет
- Jurnal Kesehatan MasyarakatДокумент8 страницJurnal Kesehatan MasyarakatDana AdwanОценок пока нет
- DownloadДокумент7 страницDownloadcesar8319Оценок пока нет
- García Hermoso2018Документ19 страницGarcía Hermoso2018Sam Steven Hernandez JañaОценок пока нет
- Health Behavior: An Overview of Effects & Issues: Jimenez, A., Beedie, C. and Ligouri, GДокумент16 страницHealth Behavior: An Overview of Effects & Issues: Jimenez, A., Beedie, C. and Ligouri, GAbdurrahamanОценок пока нет
- Am. J. Epidemiol.-2003-Ma-85-92Документ8 страницAm. J. Epidemiol.-2003-Ma-85-92Eima Siti NurimahОценок пока нет
- Hydratacion Indices Longitud Acute IJSNEM 2010Документ9 страницHydratacion Indices Longitud Acute IJSNEM 2010RosaОценок пока нет
- Nutrition and Physical Activity For Health: John M. Jakicic, PHDДокумент23 страницыNutrition and Physical Activity For Health: John M. Jakicic, PHDtimothyhwangОценок пока нет
- Effects of Low-Intensity Resistance Exercise With Vascular Occlusion On Physical Function in Healthy Elderly People.-2Документ7 страницEffects of Low-Intensity Resistance Exercise With Vascular Occlusion On Physical Function in Healthy Elderly People.-2Ingrid Ramirez PОценок пока нет
- Osteo 1Документ6 страницOsteo 1Ardhyan ArdhyanОценок пока нет
- (2017) Running Does Not Increase Symptoms or Structural Progression in People With Knee Osteoarthritis - Data From The Osteoarthritis InitiativeДокумент8 страниц(2017) Running Does Not Increase Symptoms or Structural Progression in People With Knee Osteoarthritis - Data From The Osteoarthritis Initiativecalixto1995Оценок пока нет
- Body Mass Index and Ischemic and Hemorrhagic Stroke: A Prospective Study in Korean MenДокумент7 страницBody Mass Index and Ischemic and Hemorrhagic Stroke: A Prospective Study in Korean MenSri Wahyuni HarliОценок пока нет
- Relationship Between Urban Sprawl and Physical Activity, Obesity, and MorbidityДокумент12 страницRelationship Between Urban Sprawl and Physical Activity, Obesity, and MorbidityMaría HurtadoОценок пока нет
- Grip Strength, Body CompositionДокумент8 страницGrip Strength, Body CompositionFPSMОценок пока нет
- Associations of Changes in Exercise Level With Subsequent Disability Among Seniors: A 16-Year Longitudinal StudyДокумент6 страницAssociations of Changes in Exercise Level With Subsequent Disability Among Seniors: A 16-Year Longitudinal StudymartinОценок пока нет
- Long-Term Leisure-Time Physical Activity Intensity and All-Cause and Cause-Specific Mortality: A Prospective Cohort of US AdultsДокумент12 страницLong-Term Leisure-Time Physical Activity Intensity and All-Cause and Cause-Specific Mortality: A Prospective Cohort of US AdultsANDRÉ GUIMARÃESОценок пока нет
- Physical Inactivity: Associated Diseases and Disorders: ReviewДокумент18 страницPhysical Inactivity: Associated Diseases and Disorders: ReviewJuan Pablo Casanova AnguloОценок пока нет
- 04 - Cardiometabolic Effects of High-Intensity Hybrid Functional Electrical Stimulation Exercise After Spinal Cord InjuryДокумент20 страниц04 - Cardiometabolic Effects of High-Intensity Hybrid Functional Electrical Stimulation Exercise After Spinal Cord Injurywellington contieroОценок пока нет
- Jurnal FisiologiДокумент8 страницJurnal FisiologiRFALWОценок пока нет
- Schroder 2005Документ17 страницSchroder 2005s3rinadataОценок пока нет
- Skeletal Muscle Hypertrophy After Aerobic Exercise TrainingДокумент9 страницSkeletal Muscle Hypertrophy After Aerobic Exercise TrainingAlbert CalvetОценок пока нет
- Epidemiology of MSK Impairment and DisabilityДокумент6 страницEpidemiology of MSK Impairment and DisabilityMd. Ariful IslamОценок пока нет
- Drinking Patterns and Body Mass Index in Never Smokers: National Health Interview Survey, 1997-2001Документ9 страницDrinking Patterns and Body Mass Index in Never Smokers: National Health Interview Survey, 1997-2001miculmucОценок пока нет
- Lewis Et Al - MrOS Fractures - JBMR2007Документ9 страницLewis Et Al - MrOS Fractures - JBMR2007chuckc123Оценок пока нет
- Effects of Diet, Physical Activity and Performance, and Body Weight On Incident Gout in Ostensibly Healthy, Vigorously Active MenДокумент8 страницEffects of Diet, Physical Activity and Performance, and Body Weight On Incident Gout in Ostensibly Healthy, Vigorously Active Menristi hutamiОценок пока нет
- (15435474 - Journal of Physical Activity and Health) Socioeconomic Predictors of A Sedentary Lifestyle - Results From The 2001 National Health SurveyДокумент12 страниц(15435474 - Journal of Physical Activity and Health) Socioeconomic Predictors of A Sedentary Lifestyle - Results From The 2001 National Health Surveyconstance yanОценок пока нет
- Sarcopenic Obesity Predicts Instrumental Activities of Daily Living Disability in The ElderlyДокумент10 страницSarcopenic Obesity Predicts Instrumental Activities of Daily Living Disability in The ElderlyFranchesca OrtizОценок пока нет
- Life Extension Magazine: The 10 Most Important Blood TestsДокумент6 страницLife Extension Magazine: The 10 Most Important Blood TestsJaffer AftabОценок пока нет
- WPTDay11 Cancer Fact Sheet C6 PDFДокумент3 страницыWPTDay11 Cancer Fact Sheet C6 PDFDr. Krishna N. SharmaОценок пока нет
- Acsm Current Comment: Physiology of AgingДокумент2 страницыAcsm Current Comment: Physiology of AgingTeoОценок пока нет
- Long QuizДокумент6 страницLong QuizMae EsmadeОценок пока нет
- Jama Physical ActivityДокумент3 страницыJama Physical ActivityflorОценок пока нет
- Alternative Medicine Joins The MainstreamДокумент68 страницAlternative Medicine Joins The Mainstreamccprado1Оценок пока нет
- Leisure-Time Running Reduces All-Cause and Cardiovascular Mortality RiskДокумент19 страницLeisure-Time Running Reduces All-Cause and Cardiovascular Mortality Riskmonalisa.fiscalОценок пока нет
- Jurnal ObesitasДокумент20 страницJurnal ObesitasTan Endy100% (1)
- Am J Clin Nutr 2008 Paddon Jones 1562S 6SДокумент5 страницAm J Clin Nutr 2008 Paddon Jones 1562S 6ScintaОценок пока нет
- The Female Athlete Triad: A Clinical GuideОт EverandThe Female Athlete Triad: A Clinical GuideCatherine M. GordonОценок пока нет
- Eng 2 Exercise Research PaperДокумент12 страницEng 2 Exercise Research Paperapi-534316399Оценок пока нет
- Oxandrolone in Older MenДокумент9 страницOxandrolone in Older MenJorge FernándezОценок пока нет
- Informed ConsentДокумент32 страницыInformed ConsentSara Montañez Barajas0% (1)
- Recruitment & RetentionДокумент20 страницRecruitment & Retentionjessica maria vasquez lopez100% (1)
- Part 1: Introduction Part 2: QA and Monitoring Role Part 3: Trial Monitoring Activities Part 4: Summary of Key PointsДокумент12 страницPart 1: Introduction Part 2: QA and Monitoring Role Part 3: Trial Monitoring Activities Part 4: Summary of Key PointsRenzo FernandezОценок пока нет
- Investigational New DrugsДокумент16 страницInvestigational New DrugsVirgil CendanaОценок пока нет
- Participant Safety and Adverse EventsДокумент27 страницParticipant Safety and Adverse EventsVirgil CendanaОценок пока нет
- Part 1: Introduction Part 2: Responsibilities by Role Part 3: Summary of Key PointsДокумент13 страницPart 1: Introduction Part 2: Responsibilities by Role Part 3: Summary of Key PointsFaye BaliloОценок пока нет
- MetodoДокумент20 страницMetodoSara Montañez BarajasОценок пока нет
- The Research ProtocolДокумент17 страницThe Research ProtocolHiếu NhiОценок пока нет
- A Cross Sectional Study of Fasting Serum Magnesium Levels in The Patients With Type 2 Diabetes Mellitus and Its Relation To Diabetic ComplicationsДокумент5 страницA Cross Sectional Study of Fasting Serum Magnesium Levels in The Patients With Type 2 Diabetes Mellitus and Its Relation To Diabetic ComplicationsRobert DwitamaОценок пока нет
- Pi Is 0091674917309193Документ9 страницPi Is 0091674917309193Annisa YutamiОценок пока нет
- DocДокумент14 страницDocSara Montañez BarajasОценок пока нет
- 7979 12179 1 SMДокумент2 страницы7979 12179 1 SMRobert DwitamaОценок пока нет
- Research Misconduct PDFДокумент15 страницResearch Misconduct PDFAnonymous b27E5uXlОценок пока нет
- The Relationship of Plasma Adipsin Adiponectin VasДокумент9 страницThe Relationship of Plasma Adipsin Adiponectin VasRobert DwitamaОценок пока нет
- DSC-management of Vitamin D DeficiencyДокумент17 страницDSC-management of Vitamin D DeficiencyRobert DwitamaОценок пока нет
- Nutrients: Vitamin D Intake and Risk of Type 1 Diabetes: A Meta-Analysis of Observational StudiesДокумент12 страницNutrients: Vitamin D Intake and Risk of Type 1 Diabetes: A Meta-Analysis of Observational StudiesRobert DwitamaОценок пока нет
- Assessment of Precautionary Measures Against COVID-19 in Indonesian WorkplacesДокумент8 страницAssessment of Precautionary Measures Against COVID-19 in Indonesian WorkplacesRobert DwitamaОценок пока нет
- Nutrients: Role of Gut Microbiota On Onset and Progression of Microvascular Complications of Type 2 Diabetes (T2DM)Документ26 страницNutrients: Role of Gut Microbiota On Onset and Progression of Microvascular Complications of Type 2 Diabetes (T2DM)Robert DwitamaОценок пока нет
- Guidance On How To Use QUADAS-C (v2020.03.12)Документ21 страницаGuidance On How To Use QUADAS-C (v2020.03.12)Robert DwitamaОценок пока нет
- Cardiovascular Disease Risk Factors and Anthropometry Features Among Seemingly Healthy Young AdultsДокумент6 страницCardiovascular Disease Risk Factors and Anthropometry Features Among Seemingly Healthy Young AdultsRobert DwitamaОценок пока нет
- Pro File of The Gut Microbiota of Adults With Obesity: A Systematic ReviewДокумент12 страницPro File of The Gut Microbiota of Adults With Obesity: A Systematic ReviewRobert DwitamaОценок пока нет
- Diagnosis and Management of HypocalcemiaДокумент11 страницDiagnosis and Management of HypocalcemiamdmmmОценок пока нет
- 1738-Article Text-17917-1-10-20191212Документ12 страниц1738-Article Text-17917-1-10-20191212Robert DwitamaОценок пока нет
- Phenolic Compounds Impact On Rheumatoid Arthritis, Inflammatory Bowel Disease and Microbiota ModulationДокумент39 страницPhenolic Compounds Impact On Rheumatoid Arthritis, Inflammatory Bowel Disease and Microbiota ModulationRobert DwitamaОценок пока нет
- Survival Analysis in RДокумент8 страницSurvival Analysis in RRobert DwitamaОценок пока нет
- Survival Analysis in R PDFДокумент16 страницSurvival Analysis in R PDFmarciodoamaralОценок пока нет
- Body Fluids: Fluid and ElectrolytesДокумент17 страницBody Fluids: Fluid and ElectrolytesRobert DwitamaОценок пока нет
- Body Fluids: Fluid and ElectrolytesДокумент17 страницBody Fluids: Fluid and ElectrolytesRobert DwitamaОценок пока нет
- Alpha and Beta ThalassemiaДокумент6 страницAlpha and Beta ThalassemiaSi vis pacem...100% (1)
- NCCN Guidelines For Multiple Myeloma V.3.2016 - Web Teleconference Interim Update On 12/14/15Документ3 страницыNCCN Guidelines For Multiple Myeloma V.3.2016 - Web Teleconference Interim Update On 12/14/15Robert DwitamaОценок пока нет
- DLP in Mapeh 9Документ4 страницыDLP in Mapeh 9Joan B LangamОценок пока нет
- Unit 7 - What Do You Like Doing? (1) +Документ6 страницUnit 7 - What Do You Like Doing? (1) +Ngọc BíchОценок пока нет
- Swimming, in Recreation and Sports, The Propulsion of The Body Through Water by Combined ArmДокумент7 страницSwimming, in Recreation and Sports, The Propulsion of The Body Through Water by Combined ArmDaisy La MadridОценок пока нет
- History of Football: Quick Summarywith StoriesДокумент9 страницHistory of Football: Quick Summarywith StoriesshettyОценок пока нет
- Bloom v. Clark Evidence ISOДокумент189 страницBloom v. Clark Evidence ISOmary engОценок пока нет
- Decatur-DeKalb Family YMCA Pool ScheduleДокумент2 страницыDecatur-DeKalb Family YMCA Pool ScheduleMetro Atlanta YMCAОценок пока нет
- Sport SalariesДокумент5 страницSport SalariesAndrew Taylor WoolleyОценок пока нет
- P6 Interview QuestionsДокумент4 страницыP6 Interview QuestionsLi Yinlai100% (1)
- Английский 4-Кл 1 - ТЕТРАДЬДокумент52 страницыАнглийский 4-Кл 1 - ТЕТРАДЬЯрослав СтефкинОценок пока нет
- Lamborghini Pirelli BrochureДокумент16 страницLamborghini Pirelli Brochuresharky67Оценок пока нет
- DHBB CBG (ĐĐX) 2019 L10Документ13 страницDHBB CBG (ĐĐX) 2019 L10Tuyền Nguyễn Thị ÚtОценок пока нет
- MR Protein - Powerbuilding ProgramДокумент10 страницMR Protein - Powerbuilding ProgramhassanОценок пока нет
- 1998 Campagnolo CatalogДокумент33 страницы1998 Campagnolo CatalogTango OscarОценок пока нет
- Edlebrock Pleads Guilty: The Delphos HeraldДокумент16 страницEdlebrock Pleads Guilty: The Delphos HeraldThe Delphos HeraldОценок пока нет
- Rules For The 2018 National Robotics Competition PDFДокумент4 страницыRules For The 2018 National Robotics Competition PDFJeseu Yeomsu JaliОценок пока нет
- Lasker: Move by MoveДокумент26 страницLasker: Move by MoveArturo GonzalezОценок пока нет
- Japanese CultureДокумент23 страницыJapanese CultureWaqi Je100% (1)
- Tabela Muscle 2023Документ6 страницTabela Muscle 2023Alison WinclerОценок пока нет
- Cat Competicion 2023Документ48 страницCat Competicion 2023amartirosОценок пока нет
- C-Bond Interhigh - Track Starting Lists - 21 Feb 2024Документ25 страницC-Bond Interhigh - Track Starting Lists - 21 Feb 2024ee8757388Оценок пока нет
- Best of Robert RingerДокумент211 страницBest of Robert RingerSanti Dewi Setiawan100% (6)
- Altaf CVДокумент2 страницыAltaf CVAyesha AltafОценок пока нет
- Chris Hemsworth Workout - The God of Thunder's Thor Workout TRAINДокумент15 страницChris Hemsworth Workout - The God of Thunder's Thor Workout TRAINeldelmoño luci100% (1)
- Total-Body Workbook: External Oblique Rectus AbdominisДокумент5 страницTotal-Body Workbook: External Oblique Rectus Abdominisrayk24zzzОценок пока нет
- Daily Assessment - X - Descriptive TextДокумент5 страницDaily Assessment - X - Descriptive TextnoorfitriamaliaОценок пока нет
- August 2021 - July 2022Документ12 страницAugust 2021 - July 2022Наталия ЧуйковаОценок пока нет
- FIBA Officiating SignalsДокумент6 страницFIBA Officiating SignalsAhle MaeОценок пока нет
- Untitled Presentation-2Документ47 страницUntitled Presentation-2api-442144248Оценок пока нет
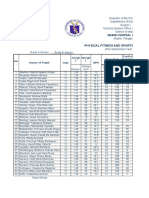
- Consolidation Physical Fitness Test FormДокумент6 страницConsolidation Physical Fitness Test Formvenus velonzaОценок пока нет
- The ICC Cricket ODI World Cup 2023 Scdule PDFДокумент4 страницыThe ICC Cricket ODI World Cup 2023 Scdule PDFShampa GhoshОценок пока нет